
Left Fascicular Blocks Simplified
How to tell if there's a Left Anterior Fascicular Block (LAFB) or a Left Posterior Fascicular Block (LPFB).

Please note: This post explains fascicular blocks, specifically the left anterior and posterior fascicular blocks (LAFB and LPFB). To read about bundle branch blocks, specifically the right and left bundle branch blocks (RBBB and LBBB), please read this post.
As if RBBB and LBBB were not enough, we also have left fascicular blocks (also known as hemiblocks).
The reason we have a left anterior fascicular block (LAFB) and a left posterior fascicular block (LPFB) is that the left bundle branch is divided into an anterior and a posterior segment (fascicle).
In addition to the anterior and posterior fascicles, a middle or septal fascicle can be recognised in the left ventricular conduction system, which might have functional and clinical significance (however, this is outside the scope of this post).
Things that you need to know first
To better understand this post, you will need to know the following:
How to identify the QRS axis (check out part 1 and part 2 of the “How to Find the QRS Axis in Under 3 Seconds With 100% Accuracy” posts) - check out this ECG simulation tool as well to help you understand the QRS axis better
How to identify RBBB and LBBB (check out this post)
Anatomy of the left anterior and posterior fascicles
The left bundle branch is divided into an anterior and a posterior fascicle. The anterior fascicle runs along the front of the left ventricle towards the anterior papillary muscle (which is located superiorly), while the posterior fascicle travels to the posterior papillary muscle (which is located inferiorly).
***What you need to remember is that the left anterior fascicle runs towards the superior part of the LV, whereas the left posterior fascicle runs towards the inferior part of the LV.
Left ANTERIOR fascicle → SUPERIOR part of LV
Left POSTERIOR fascicle → INFERIOR part of LV
Normally, conduction through both fascicles occurs simultaneously, resulting in uniform electrical activation of the left ventricle. However, if conduction is blocked in one of the fascicles, initial depolarization of the left ventricle arises solely from the unaffected fascicle.
Similarly to bundle branch blocks, there are fascicular blocks.
The left fascicular blocks are an “up-down” problem
This is in contrast with bundle branch blocks, which are a right-left problem (see what this means in this post about RBBB and LBBB).
Let’s orient ourselves a little bit with the images that we are going to see below.
The parasternal long axis (PLAX) view during echocardiography captures the section of the heart shown in the following image.

In this view, you can see the anterior and posterior walls of the left ventricle. The drawings of the heart that follow are based on this view.

Here, you can see that the anterior papillary muscle (where the left anterior fascicle goes) is located more superiorly than the posterior papillary muscle (where the left posterior fascicle goes).
Therefore, because of this anatomy, fascicular blocks (LAFB and LPFB) are an up-down problem.
To view both the superior and inferior parts of the heart simultaneously, you need to look at it in the frontal plane. Which leads “look” at the heart in the frontal plane? The limb leads.
Specifically, we need one lead that ‘looks’ at the superior part of the LV and one that looks at the inferior part LV. These are the following:
aVL: “looks” at the superior part of the LV (at -30 degrees)
aVF: “looks” at the inferior part of the LV (at +90 degrees)
So, to tell if there is a QRS pattern consistent with a fascicular block, you only need to look at aVL and aVF.
Left anterior fascicular block (LAFB)
In LAFB, the left ventricle is activated first by the left posterior fascicle, resulting in initial impulses directed downward (towards the posterior papillary muscle). This causes an initial small positive deflection in aVF and a negative deflection in aVL.
***The red arrows in the following images represent the sum of all the electrical forces' vectors at a specific time point.

As depolarization spreads toward the blocked superior region of the left ventricle (through slower myocyte-to-myocyte conduction), a larger positive deflection is created in lead aVL, while a negative deflection develops in aVF. This abnormal activation results in LEFT axis deviation.
***Note: not just a LEFT axis deviation (which is between −30° and −90°), but a significant LEFT axis deviation (which is between −45° and −90°).

Overall, LAFB creates a qR pattern in aVL and an rS pattern in aVF.
Left posterior fascicular block (LPFB)
A left posterior fascicular block (LPFB) is less common than a left anterior fascicular block (LAFB).
With an LPFB, the ventricle is activated by the left anterior fascicle alone, causing the initial forces to be directed upward (towards the anterior papillary muscle). This creates an initial small negative deflection in aVF and a positive deflection in aVL.

Subsequently, as the impulse spreads downward toward the initially blocked region (through myocyte-to-myocyte conduction again), a larger positive is created in aVF while a negative deflection is recorded in aVL. This causes RIGHT axis deviation.
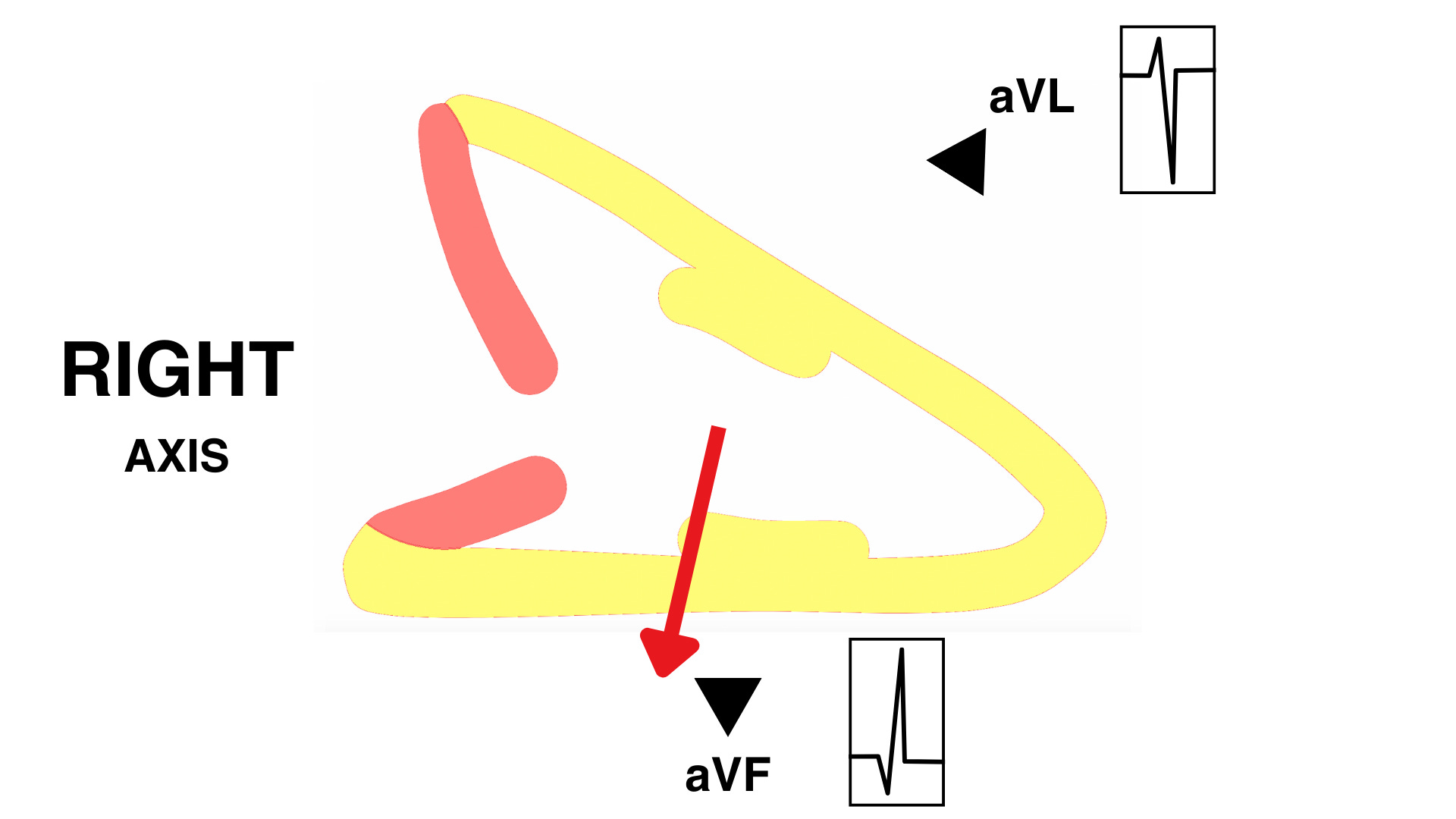
Overall, LPFB creates a rS pattern in aVL and an qR pattern in aVF.
LAFB and LPFB ECG criteria

If you don’t know or remember what the “R wave peak time” is, please read my post on RBBB and LBBB, where I explain it.
Differences between bundle branch blocks and left fascicular blocks
1) Limb leads VS precordial leads
As explained earlier, to diagnose RBBB and LBBB, you only look at the precordial leads (specifically, V1 and V6).
On the other hand, to diagnose LAFB and LPFB, you only look at the limb leads (specifically, for simplicity, aVL and aVF).
2) QRS duration
Unlike RBBBs and LBBBs, LAFB and LPFB do not cause significant widening of the QRS because the Purkinje fibres, which conduct rapidly, bridge the territories served by the anterior and posterior fascicles. Therefore, the QRS duration, although slightly prolonged, should not be more than 120 msec in fascicular blocks.
3) QRS axis deviation
When I first started learning about bundle branch blocks, I had the impression that RBBB causes right axis deviation and LBBB causes left axis deviation. I've noticed that other people have the same impression as well.
This is incorrect. RBBB does NOT necessarily cause right axis deviation, and similarly, LBBB does NOT necessarily cause left axis deviation.
However, fascicular blocks DO cause axis deviation (ALWAYS) - see above why. Specifically:
LAFB → LEFT axis deviation (between −45° and −90°)
LPFB → RIGHT axis deviation
Summary
Now that you know how to diagnose RBBB, LBBB, LAFB, and LPFB, you essentially know everything you need to know about IVCD (interventricular conduction delay - some people call it intraventricular conduction delay, and these terms are interchangeable).
To sum up, let's take a look at the diagnostic criteria for all of these abnormalities in a single table:

References
Lilly, L. S. (2021). Pathophysiology of Heart Disease (7th ed.). Wolters Kluwer.
Surawicz B, Childers R, Deal BJ, Gettes LS. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram, part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Circulation. 2009;119:e235–e240
Pérez-Riera AR, Barbosa-Barros R, Daminello-Raimundo R, de Abreu LC, Tonussi Mendes JE, Nikus K. Left posterior fascicular block, state-of-the-art review: A 2018 update. Indian Pacing Electrophysiol J. 2018 Nov-Dec;18(6):217-230. doi: 10.1016/j.ipej.2018.10.001. Epub 2018 Oct 13. PMID: 30326266; PMCID: PMC6302819.
Gao Y, Xia L, Gong YL, Zheng DC. Electrocardiogram (ECG) patterns of left anterior fascicular block and conduction impairment in ventricular myocardium: a whole-heart model-based simulation study. J Zhejiang Univ Sci B. 2018 Jan.;19(1):49-56. doi: 10.1631/jzus.B1700029. PMID: 29308607; PMCID: PMC5802974.
Scherbak D, Hicks GJ. Left Bundle Branch Block. [Updated 2023 Feb 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482167/