

Premature Complexes: Atrial vs Ventricular
Understanding the difference between different types of premature complexes and why it matters


Normally, myocardial depolarisation starts from the sinoatrial node (SA node). This has the following two consequences on the 12-lead ECG:
atrial depolarisation occurs from top to bottom, shown with a positive P wave in the inferior leads (II, III, aVF) and a negative P wave in aVR.
atrial depolarisation precedes ventricular depolarisation, shown with a P wave preceding the QRS complex.
Occasionally, myocardial cells from other areas can fire prematurely and spread their electrical signals to the rest of the myocardium.
In these circumstances, the depolarization of the myocardium is not initiated by the sinoatrial (SA) node but by a different focus. Depending on the location of this focus, two different ECG patterns can be observed:
Premature atrial complexes: the focus originates from the atria
Premature ventricular complexes: the focus originates from the ventricles
Premature atrial complexes (PACs)
There is always a preceding P wave before the QRS complex.
The P wave has different morphology than the normal sinus P wave (unless it originates from an area very close to the SA node, in which case it may be indistinguishable from a sinus P wave on a 12-lead transthoracic ECG).
The PR interval is probably different as well (remember: the P wave and PR interval “go together”).
The QRS complex is usually narrow but could be broad as well. The QRS is the same as the rest of the QRS complexes of the same ECG. If the patient has a narrow QRS normally, then the QRS of the premature complex will be narrow as well. If the patient has underlying LBBB, then the QRS of the ectopic will have an LBBB morphology as well. There are two exceptions to this rule:
The PAC occurs very early and encounters the right bandle branch in its refractory period, therefore conducting to the ventricles only through the left bundle branch (i.e. with an RBBB).
The PAC occurs too early, and both the right and left bundle branches are in a refractory state, therefore not conducting to the ventricles and not producing a subsequent QRS complex altogether. In this case, you will only see a P wave without conducting to the ventricles.
Premature ventricular complexes (PVCs)
There is no preceding P wave (and so no PR interval either).
The QRS complex is always broad, as the PVCs originate from the ventricles and do not follow the normal pathway for depolarising the ventricles (but a different, slower one).
As the QRS is broad and abnormal, expect to see abnormal ST segment and T wave as well (the depolarisation of the ventricles affects their repolarisation as well).
Summary
Here is a table summarising key information about premature complexes:
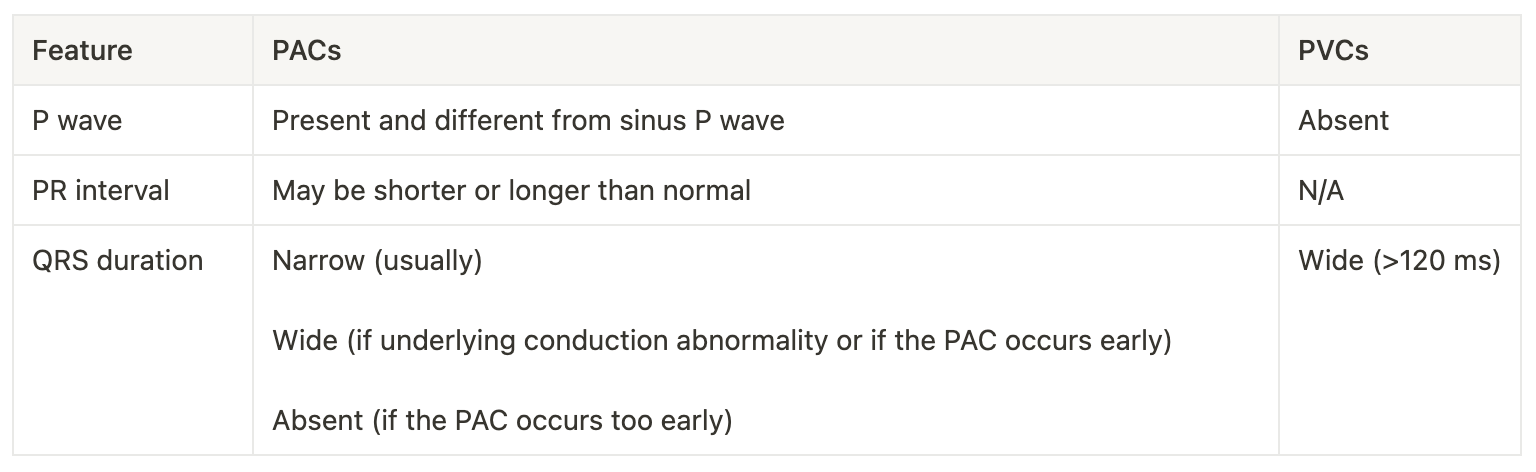
Example
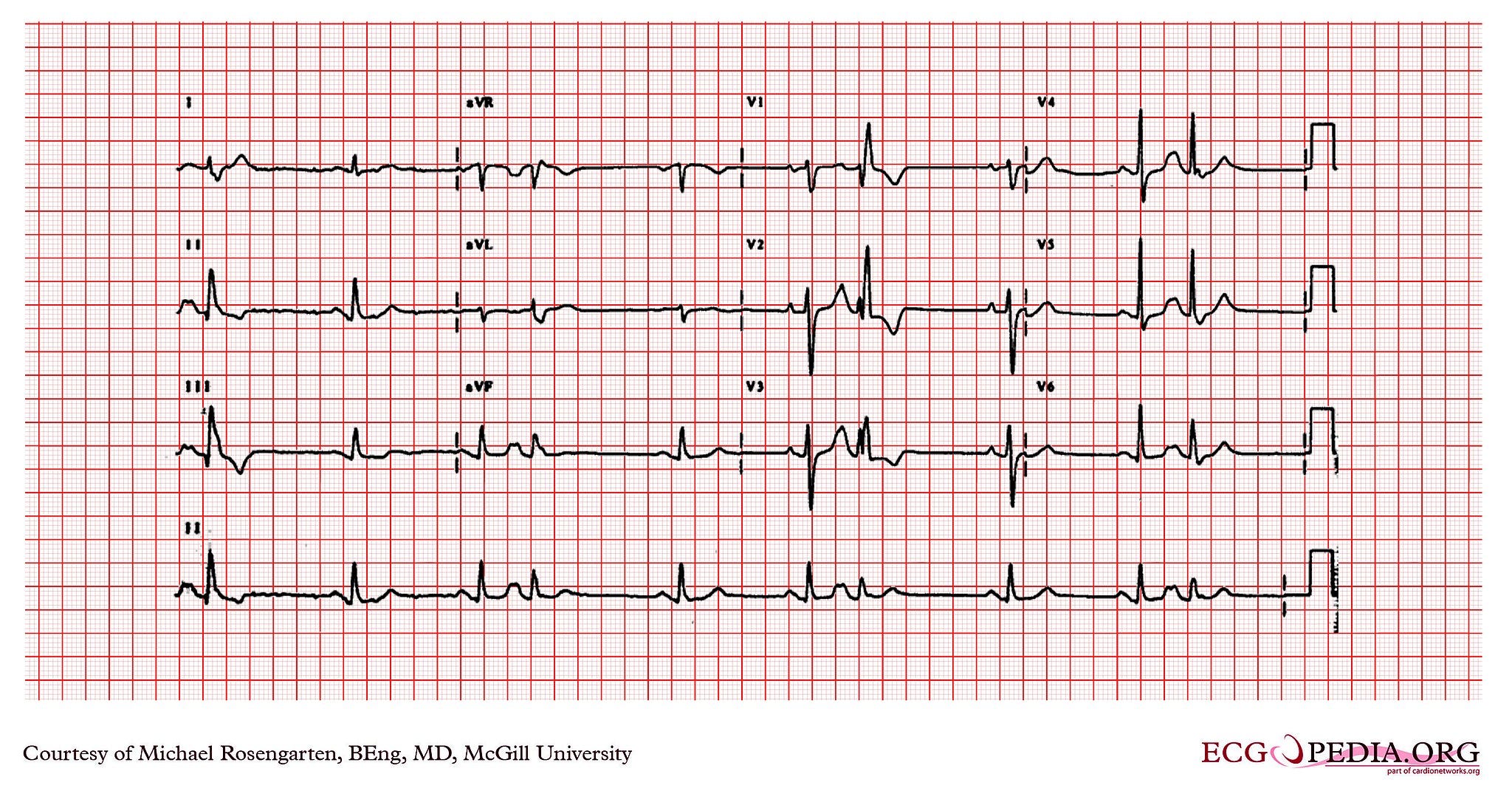
Michael Rosengarten BEng, MD.McGill, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
In the case above, you can see several PACs that come very early, therefore producing a wide QRS complex with an RBBB morphology. You can see the premature P waves buried inside the previous T waves (tip: compare the T waves with each other). So, despite that the QRS is wide, these are not PVCs but PACs.
And that's not all...
In addition, there are premature junctional complexes (originating from the AV node or the bundle of His). These generally look like PACs, but they are uncommon. Therefore, I will not write about them in this article (perhaps in a future article).
Question for you
What is the compensatory pause, and how is it different between PACs and PVCs? You can send me an email with your answer!
I hope you have a wonderful weekend! If you have any questions or feedback, please leave a comment.
If you know anyone who could benefit from this newsletter, please share it with them.
Disclaimer
The information in this newsletter is for educational purposes only and is not intended to substitute for professional medical advice, diagnosis, or treatment. The content is based on general ECG interpretation principles and may not apply to every patient case. Readers should always seek the advice of a qualified healthcare provider with any questions or concerns they may have regarding a medical condition. The author and publisher of this newsletter are not liable for any damages or injuries arising from the use or misuse of the information presented in this newsletter. While every effort has been made to ensure the accuracy and completeness of the information provided, the author and publisher make no warranties or representations, expressed or implied, about the accuracy, reliability, or suitability of the content. The author and publisher disclaim any liability or responsibility for any errors or omissions in the content or for any loss or damage of any kind arising directly or indirectly from the use or reliance on the information provided.