

Low QRS Voltage (LQRSV): Why All ECG Interpreters Should Know About It
Low QRS Voltage (LQRSV): Why All ECG Interpreters Should Know About It
Everything you need to know about what LQRSV is and its causes!

What is low QRS voltage (LQRSV)?
Simply put:
QRS amplitude ≤5mm (0.5 mV) in all limb leads OR
QRS amplitude ≤10mm (1.0 mV) in all precordial leads
The QRS amplitude is measured from the highest to the lowest point of the QRS.
Please note that the measurements in mm apply ONLY in standard calibration (i.e. 10 mm/mV).
Take a look at the following ECG for example:

In the ECG above, there’s no single limb lead with a QRS voltage greater than 5 mm. This is a typical example of LQRSV.
But why should you know about LQRSV? To answer this question, we need to delve deeper into its causes.
The aetiology of LQRSV
Think of the QRS voltage as the loudness of the ventricles’ voice.
Is the ventricles’ voice weak (is there a problem with the ventricular myocardium itself)?
→ Impaired voltage generation
Or maybe someone else is covering their mouth so they’re not heard (is there something opposing signal transmission around the ventricular myocardium)?
→ Increased impedance
A) Impaired voltage generation
There’s something wrong with the ventricular myocardium that weakens its voice. Typical causes include:
1. Cardiomyopathy
We start with this one because it’s extremely important.
Actually, it’s not “one”, as cardiomyopathy is a spectrum of diseases (some of them being spectrums themselves), including, but not limited to, hypertrophic cardiomyopathy (HCM), arrhythmogenic cardiomyopathy (ACM), and dilated cardiomyopathy (DCM).
The definition of cardiomyopathy is the following:
“A myocardial disorder in which the heart muscle is structurally and functionally abnormal, in the absence of coronary artery disease, hypertension, valvular disease and congenital heart disease sufficient to cause the observed myocardial abnormality.”²
As the cardiac muscle is not working “properly”, it may not generate normal electrical impulses (i.e. QRS voltage).
Why is it important? Sudden cardiac death (SCD) is commonly due to coronary artery disease (CAD) in people of age > 35. However, for people younger than 35, the most common cause is sudden unexplained death (SUD). In this group of causes, cardiomyopathies play a significant role.
Cardiomyopathies have been reported to be 15-30% of the causes of SCD in young people (age < 35).
When you see LQRSV and repolarization abnormalities, such as T-wave inversion, this is a red flag and should prompt you to investigate it further. It might be an initial expression of a cardiomyopathy.
And note that occasionally the first clinically significant expression of a cardiomyopathy will be SCD!
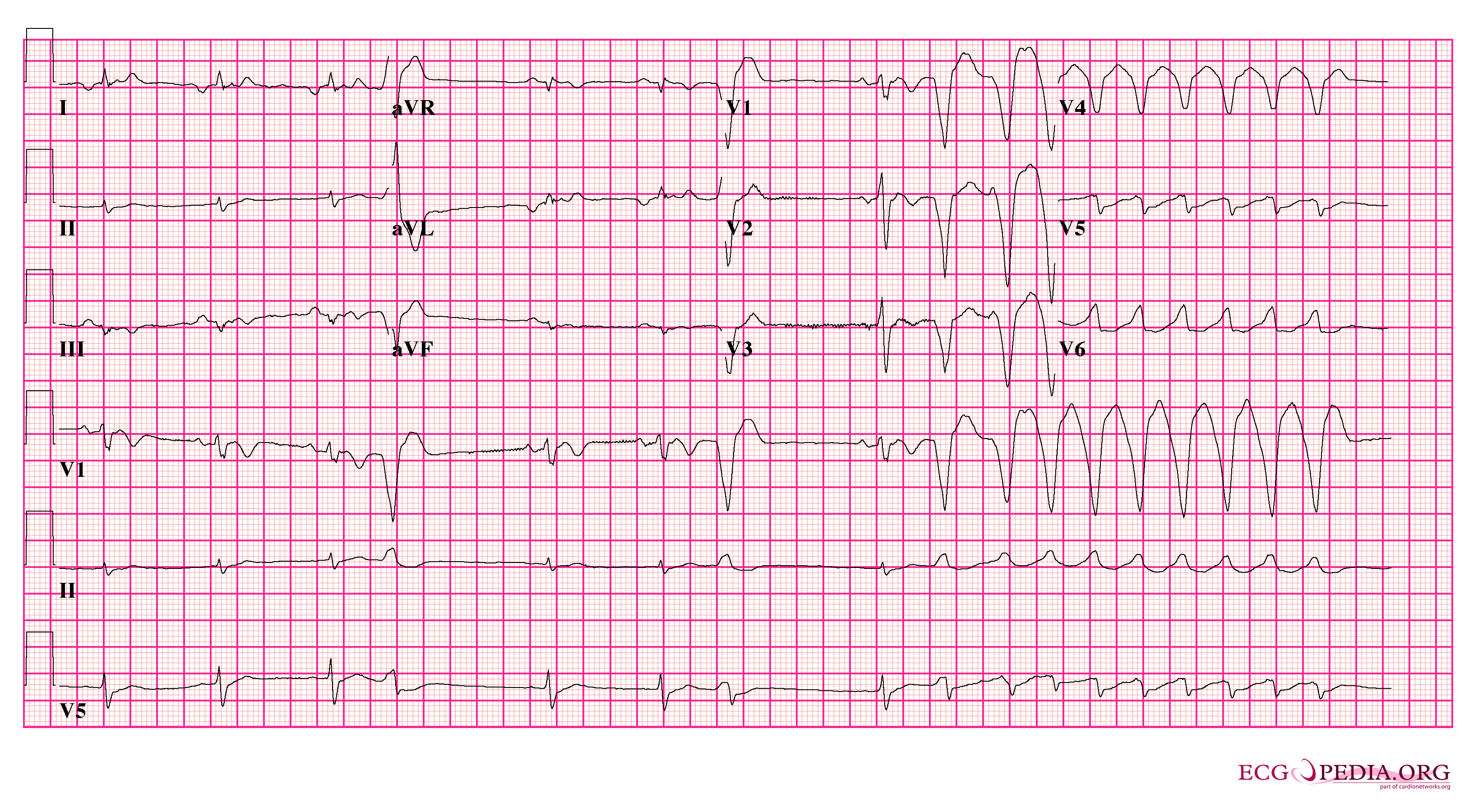
The ECG above has quite a few abnormalities, but we’ll focus on two: low QRS voltage in the limb leads and T-wave inversion in V1-V3. This is arrhythmogenic cardiomyopathy (ACM). You can see two premature ventricular complexes (PVCs), and then you see the start of ventricular tachycardia (VT).
2. Myocardial infarction (MI)
Myocardial infarction is the process of formation of a myocardial infarct, i.e. dead myocardial tissue, which is electrically inert. Therefore, the sum of the electrical force of the myocardium is reduced, reducing the QRS voltage as well.
3. Heart failure
A myocardium that fails to contract normally will also fail to generate normal electrical impulses.
4. Myocarditis
B) Increased impedance
1) …due to air
(meaning, increased impedance because there is increased air in between the heart and the skin electrodes)
Pneumopericardium (air in the pericardial cavity)
Pneumothorax (air in the pleural cavity)
Pneumomediastinum (air in the mediastinum)
COPD (emphysema = hyperinflated lungs)
2) …due to fluid
(meaning, increased impedance because there is increased fluid in between the heart and the skin electrodes)
Pericardial effusion (increased fluid in the pericardial cavity) and cardiac tamponade (pericardial effusion that’s become life-threatening)
LQRSV and sinus tachycardia should raise suspicion about pericardial effusion with cardiac tamponade.
Why is sinus tachycardia important in this case? This post about sinus tachycardia provides essential insights into human physiology that will help you understand the causes of sinus tachycardia.If you combine the above (LQRSV and sinus tachycardia) with electrical alternans, you will get a highly specific (but modestly sensitive) pattern for cardiac tamponade.
Electrical alternans is when the QRS voltage changes from beat to beat. This happens when there’s such a large pericardial effusion that the heart literally swings every time it beats, therefore changing the QRS axis (see the ECG at the end of this section)!
Pleural effusion (fluid in the pleural cavity)
Pulmonary oedema (fluid inside the alveoli)
Peripheral oedema (interstitial fluid)
3) …due to electrically inert tissue
(meaning, increased impedance because there is increased electrically inert tissue in between the heart and the skin electrodes)
Obesity (fat tissue)
Constrictive pericarditis (granulation tissue in the pericardium)
The ECG above shows characteristic findings of cardiac tamponade:
Low QRS voltage (seen here as QRS voltage < 10 mm in all the precordial leads)
Electrical alternans (changes in the QRS voltage from beat to beat)
Tachycardia (often this is the most important sign that the heart is struggling, especially when it’s sinus tachycardia)
Things to keep in mind
The absence of LQRSV doesn’t exclude any of the diseases above.
Similarly, LQRSV is occasionally thought to be a normal variant if not associated with other ECG abnormalities in healthy individuals with a negative family history of SCD.
Beyond its diagnostic value, LQRSV has a prognostic role in clinical practice and has been demonstrated to be associated with increased mortality in individuals free of any cardiovascular disease.
Summary
In this post, we've delved into Low QRS Voltage (LQRSV), a crucial aspect of ECG interpretation. Here are the key takeaways:
LQRSV is a condition where the QRS amplitude is:
≤5mm in all limb leads OR
≤10mm in all precordial leads
The causes of LQRSV can be broadly divided into two categories according to the cause’s mechanism (occasionally, it’s a normal variant):
impaired voltage generation
increased impedance
It’s crucial to be aware of the potential causes of a low voltage, especially when combined with repolarization abnormalities, such as T-wave inversion, as this points towards a cardiomyopathy. This can be seen in an otherwise healthy young individual.
Here is a table summarising the causes of LQRSV:

Thanks for reading!
I hope you found this post useful! If so, please consider leaving a comment, a like and sharing with someone else who might find it helpful. This will help me a lot to continue writing posts like this one. Thank you!
References
Francesca Valentini and others, Diagnostic and prognostic value of low QRS voltages in cardiomyopathies: old but gold, European Journal of Preventive Cardiology, Volume 29, Issue 8, May 2022, Pages 1177–1187, https://doi.org/10.1093/eurjpc/zwaa027
Perry Elliott and others, Classification of the cardiomyopathies: a position statement from the European Society of Cardiology working group on myocardial and pericardial diseases, European Heart Journal, Volume 29, Issue 2, January 2008, Pages 270–276, https://doi.org/10.1093/eurheartj/ehm342
Katja Zeppenfeld and others, 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Developed by the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) Endorsed by the Association for European Paediatric and Congenital Cardiology (AEPC), European Heart Journal, Volume 43, Issue 40, 21 October 2022, Pages 3997–4126, https://doi.org/10.1093/eurheartj/ehac262
Abbas R, Abbas A, Khan TK, Sharjeel S, Amanullah K, Irshad Y. Sudden Cardiac Death in Young Individuals: A Current Review of Evaluation, Screening and Prevention. J Clin Med Res. 2023 Jan;15(1):1-9. doi: 10.14740/jocmr4823. Epub 2023 Jan 24. PMID: 36755763; PMCID: PMC9881489.