
Ashman phenomenon | ECG challenge #5
When seeing a broad QRS complex in atrial fibrillation with a rapid ventricular response, think “Ashman phenomenon”.

Clinical case
A 68-year-old man has palpitations and mild breathlessness for several hours. He has a history of hypertension and paroxysmal atrial fibrillation.
He reports no chest pain or syncope. Cardiovascular examination reveals an irregularly irregular rhythm.
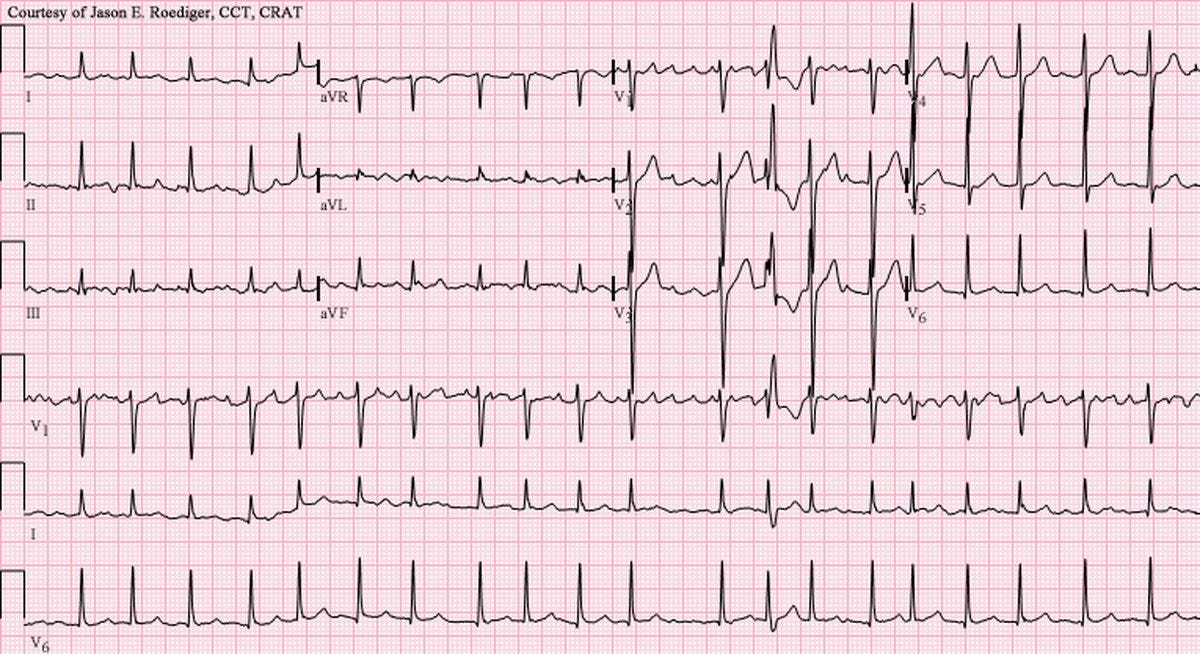
An image of a 12-lead ECG is provided below.
ECG systematic analysis
Although the paper recording speed and voltage calibration are not reported, we’ll assume it to be 25 mm/s, and 10 mm/mV, respectively (standard).
This ECG shows the following:
Rhythm: Atrial fibrillation, as seen by the irregularly irregular rhythm.1
P waves: N/A (as the rhythm is atrial fibrillation)
PR interval: N/A (as the rhythm is atrial fibrillation - no P waves → no PR interval)
QRS complex:
Duration: Less than 120 ms, except for the thirteenth (13th) QRS complex, which is prolonged (around 140 msec).
Axis: Positive in leads I and II; therefore, the QRS axis is normal.
Morphology: Normal, except for the thirteenth (13th) QRS complex which has an RBBB morphology shown by the rSR’ pattern in lead V1 and RS (wide S) pattern in the bottom rhythm strip which is V6. This complex has a short R-R interval with the previous one, and the previous one has a long R-R interval with the one before that. This is consistent with Ashman’s phenomenon.
Voltage: Normal
QT interval: 442 ms (QTcB)
ST Segment: 1 mm ST depression anterolaterally, likely rate-related
T waves: Normal
Overall, atrial fibrillation with a rapid ventricular response and a single wide-QRS complex.
Correct answer
The correct answer is aberrant conduction.
This is when an atrial impulse conducted during a relative refractory period after a long-short RR interval (Ashman phenomenon).
The ECG demonstrates atrial fibrillation with a single wide QRS complex that displays a right bundle branch block (RBBB) morphology (13th beat), specifically following a long RR interval succeeded by a short RR interval. This pattern is characteristic of the Ashman phenomenon. Basically, this means that this is a complex which occurred due to aberrant conduction (rate-related block).
The underlying mechanism is that, during atrial fibrillation, the refractory period of the His-Purkinje system is rate-dependent: it lengthens after a long RR interval (slow heart rate) and shortens with a faster rate. When a short-coupled atrial impulse follows a long RR interval, the right bundle branch may still be in its relative refractory period, resulting in transient aberrant conduction and a wide QRS complex with RBBB morphology. This is a classic example of rate-related block, and it is most commonly seen in atrial fibrillation due to the highly variable RR intervals.
I think of this mechanism as follows:
During AF, the bundle branches try to adapt to the irregular timing of signals. After a longer pause, the right bundle “relaxes” a bit too much—so when the next signal comes sooner than expected, it catches the right bundle off guard, leading to a temporary block and a wide QRS.2
Incorrect options:
Fixed anatomical RBBB – A fixed block would result in a persistent RBBB morphology on every QRS complex, not just a single wide complex.
Premature ventricular complex – A PVC would also cause a wide QRS complex, but it’s usually followed by a compensatory pause and isn’t usually associated with a preceding long-short RR interval. There could be an interpolated PVC (one without a compensatory pause), but the picture of atrial fibrillation with a rapid ventricular response and the preceding long-short RR interval suggests Ashman phenomenon is the most likely explanation.
Ventricular preexcitation – Preexcitation syndromes, such as Wolff-Parkinson-White, produce a delta wave and a consistently short PR interval, not an isolated wide QRS complex with RBBB morphology following a long-short RR interval.
Summary
Recognising Ashman phenomenon is useful because it helps differentiate between a supraventricular beat with aberrant conduction and a premature ventricular complex (PVC).
Further reading
Grigg WS, Pearlman JD, Nagalli S. Ashman Phenomenon. [Updated 2024 Sep 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562311/
There is some visible atrial activity, especially in lead V1, consistent with coarse atrial fibrillation (f waves). The f-f interval is not constant and also the morphology of each f wave is not the same, therefore all of these features are consistent with atrial fibrillation (as opposed to atrial flutter where the flutter-to-flutter interval should be constant and at around 300 bpm).
Please note that in most people the right bundle branch has a longer refractory period than the left, that's why, usually, in rate-related block, the QRS morphology is that of an RBBB.