

How Bad Can Alcohol Be for Your Heart?
Alcohol is always more insidious than we think it is...


How can drinking affect your breathing?
Approximately 18 months ago, I was asked to review a new admission in Cardiology: a gentleman in his fifties who had been admitted with progressive dyspnoea.1
PMHx: nil
PCHx:
Progressive dyspnoea over the last 5 weeks. Initially, he noticed that he was becoming dyspnoeic on exertion and then when he would lie flat. He would wake up in the middle of the night gasping for air.
In the last few days prior to his admission, he had been prescribed salbutamol for possible bronchospasm (decided after telephone consultation; note that this was during the second lockdown where getting seen by a GP was extremely challenging - this was the worst wave of COVID-19).
He was in a terrible state: he had to be standing, leaning and resting his arms on a wall to breathe properly.
I remember him telling me, “I think this inhaler that the GP gave me made me feel worse.”
He also had a non-productive cough that was getting progressively worse.
He did not have chest pain, presyncope/syncope, palpitations, pyrexia or other symptoms consistent with an infection.
Social Hx:
He lived alone, was independent and didn’t smoke. He did make a major lifestyle change two years prior, though. He had started drinking, consuming more than 10 units of alcohol per day for the last two years.
On examination:
He was sat up in bed and looked very dyspnoeic. He couldn’t speak in complete sentences and was using accessory respiratory muscles. The more he tried to talk, the more he became breathless and the more he was coughing.
His heart rate was rapid and irregular, so it was challenging to auscultate for heart sounds and listen for murmurs.
On lung auscultation, he had reduced air entry bi-basally and crackles in the mid-zones bilaterally.
His JVP was elevated, and he had bilateral peripheral pitting oedema up to his knees.
No other significant findings were noted.
His ECG looked like this:

And his chest XR was like this:

His transthoracic echocardiogram (TTE) showed a left ventricular ejection fraction of 15% (although this wasn't very accurate in the context of a rapid heart rate)!
What happened?
In summary, a patient in his fifties, with no previously diagnosed health problems and no regular medications, presented with acute heart failure. Why?
The lifestyle change of excessive alcohol consumption added a significant risk factor for the patient. Could this have caused all this?
What can alcohol do to our hearts?
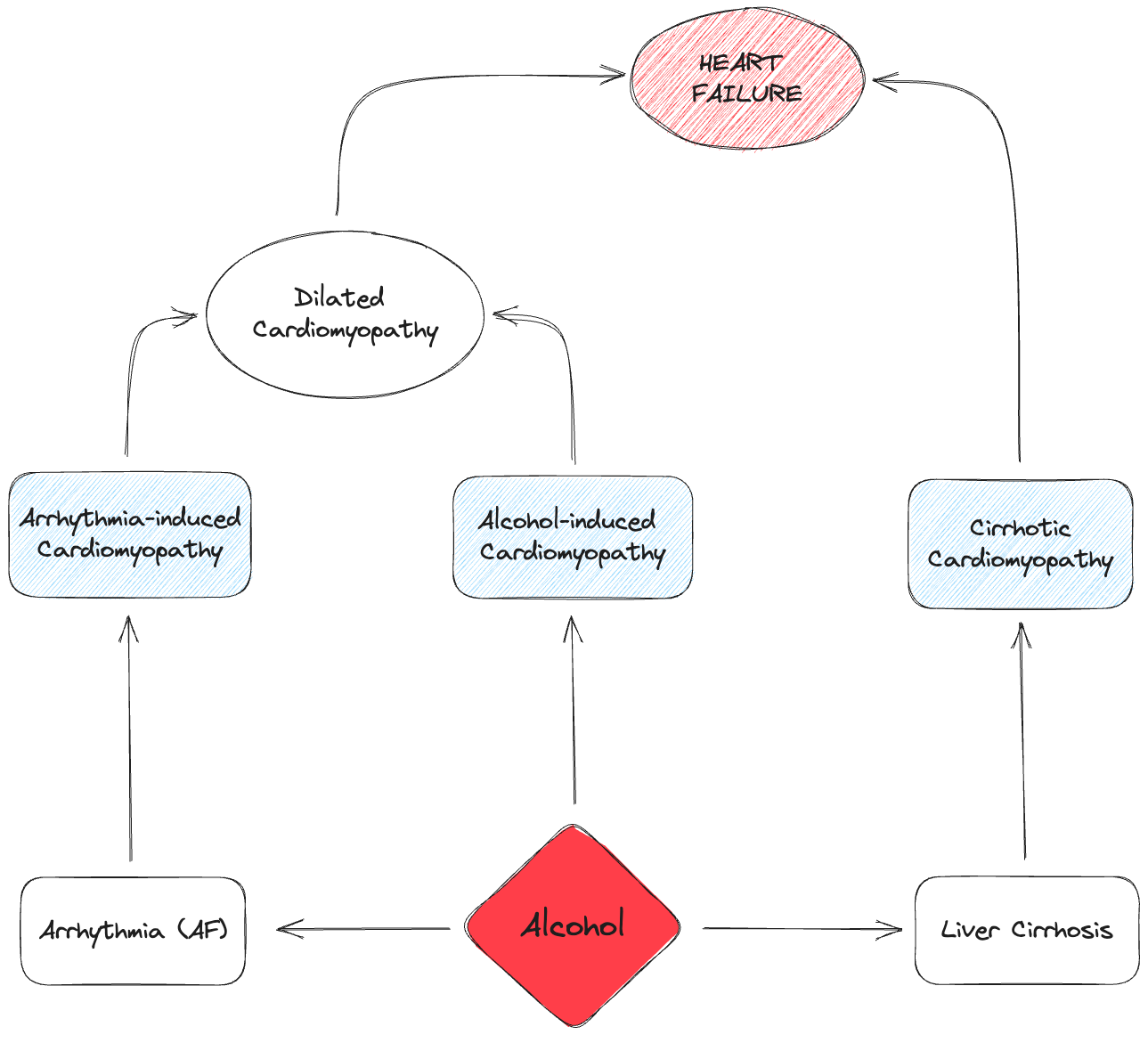
Alcohol consumption can cause heart failure in (at least) the following three different ways:
Direct myocardial damage from alcohol
Through causing arrhythmias, most commonly atrial fibrillation
Through causing liver cirrhosis
In the first two ways, alcohol can lead to the development of dilated cardiomyopathy (DCM).
Let’s dive in and see the above in more detail.
Dilated Cardiomyopathy (DCM)
As per the most recent ESC 2023 guidelines on Cardiomyopathies, dilated cardiomyopathy (DCM) is defined as follows: [1]
Left ventricular (LV) dilatation
Global or regional systolic dysfunction
The above is to be unexplained solely by abnormal loading conditions (e.g. hypertension, valve disease, congenital heart disease) or coronary artery disease
Right ventricular (RV) dilatation and dysfunction may be present as well.
Causes of DCM include stress, infections, toxins, genetics, pregnancy, tachycardia, sarcoidosis, end-stage kidney disease, autoimmune disease, endocrine dysfunction, and nutritional deficiencies. [2]

Alcohol-induced cardiomyopathy
Alcohol can cause direct damage to the myocardium and eventually lead to a type of dilated cardiomyopathy known as alcohol-induced cardiomyopathy.
Prolonged alcohol excess is required to make the diagnosis. Specifically, you’d expect a patient to be drinking more than 80g (6 units, or 3 pints of beer) daily over a period of at least 5 years to develop this type of cardiomyopathy. [3]
Arrhythmia-induced cardiomyopathy
Prolonged periods of rapid ventricular heart rates can cause another type of dilated cardiomyopathy known as arrhythmia-induced cardiomyopathy.
It takes months to develop.
Thankfully, it often improves or resolves completely following treatment and is associated with a good prognosis in most patients. [4]
Atrial fibrillation (AF) plays an extremely important role in the development of arrhythmia-induced cardiomyopathy because it can result in rapid ventricular heart rates.
The obvious connection I’d like to make here is the following:
Alcohol → AF → rapid ventricular response (for months) → arrhythmia-induced cardiomyopathy
Alcohol is a risk factor for the development of new AF but also an acute trigger of AF episodes.
Up to 60% of binge drinkers with or without underlying alcohol-induced cardiomyopathy have AF. Most cases occur during and following weekends or holidays when alcohol intake is increased (holiday heart syndrome).
Even small amounts of alcohol (one to two drinks) can trigger AF in some people. [5]
Cirrhotic cardiomyopathy
Studies have found that cirrhosis is associated with independent myocardial dysfunction, regardless of alcohol exposure.
In cirrhotic cardiomyopathy, you have a chronic cardiac dysfunction in patients with cirrhosis that you cannot explain otherwise. This condition is characterised by:
impaired contractile responsiveness to stress and/or
diastolic dysfunction
Unlike alcohol-induced cardiomyopathy, the cardiomyopathy of cirrhosis can only be improved by restoring adequate liver function, either through liver recovery or transplantation.
Cirrhotic cardiomyopathy doesn't meet the criteria for DCM, as the left ventricular cavity size is generally normal, although dilatation might be seen in some cases. [2]
Summary
Alcohol can cause heart failure.
Alcohol is always more insidious than we think it is…
Thanks for reading!
References
Elena Arbelo, Alexandros Protonotarios, Juan R Gimeno, Eloisa Arbustini, Roberto Barriales-Villa, Cristina Basso, Connie R Bezzina, Elena Biagini, Nico A Blom, Rudolf A de Boer, Tim De Winter, Perry M Elliott, Marcus Flather, Pablo Garcia-Pavia, Kristina H Haugaa, Jodie Ingles, Ruxandra Oana Jurcut, Sabine Klaassen, Giuseppe Limongelli, Bart Loeys, Jens Mogensen, Iacopo Olivotto, Antonis Pantazis, Sanjay Sharma, J Peter Van Tintelen, James S Ware, Juan Pablo Kaski, ESC Scientific Document Group , 2023 ESC Guidelines for the management of cardiomyopathies: Developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC), _European Heart Journal_, 2023;, ehad194, [https://doi.org/10.1093/eurheartj/ehad194](https://doi.org/10.1093/eurheartj/ehad194
Marilyn Weigner, MD, FACCJames P Morgan, MD, PhD. Causes of dilated cardiomyopathy. Post TW, ed. In: UpToDate, Post, TW (Ed), UpToDate, Waltham, MA, 2023.
Ihsan M Rafie, MRCP, Wilson S Colucci, MD. Alcohol-induced cardiomyopathy. Post TW, ed. In: UpToDate, Post, TW (Ed), UpToDate, Waltham, MA, 2022.
Cynthia M Tracy, MD. Arrhythmia-induced cardiomyopathy. Post TW, ed. In: UpToDate, Post, TW (Ed), UpToDate, Waltham, MA, 2022.
David Spragg, MD, FHRS. Epidemiology, risk factors, and prevention of atrial fibrillation. Post TW, ed. In: UpToDate, Post, TW (Ed), UpToDate, Waltham, MA, 2023.
Disclaimer: This story is based on a true event; however, to protect the privacy and anonymity of the patient, certain details have been altered.