

The Hidden Danger of Inferior STEMI
The Hidden Danger of Inferior STEMI
When finding an inferior STEMI, your diagnostic work doesn’t end there; here’s why.

I recently posted two questions for you, inspired by my recent post about the connection between STEMI and AV block.
You can find the questions here.
Please take a quick look and try to answer the quiz below:
RCA: Right Coronary Artery
Remember: when referring to a STEMI region, we usually mean the left ventricle unless otherwise stated. This means that if we say "anterior STEMI", we are referring to a STEMI of the anterior wall of the LEFT VENTRICLE.
Thank you for answering the questions above! If you liked the quiz, please consider subscribing and sharing.
Let's dive straight into answering the questions.
Question 1: Which of the following structures is (most commonly) perfused by the RCA
The answer here is the Right Ventricle.
So far, we know that the RCA supplies the following:
the Right Ventricle (RV)
the inferior wall of the Left Ventricle (LV) (in 85% of the population) - in which case the coronary circulation is termed right dominant
the AV node (in 90% of the population)
the SA node (in 60% of the population)
Question 2: Which STEMI pattern is most commonly associated with occlusion of the RCA?
The answer here is Inferior STEMI.
Take a look at the anatomy of the coronary arteries, and specifically the RCA, in the following picture.1
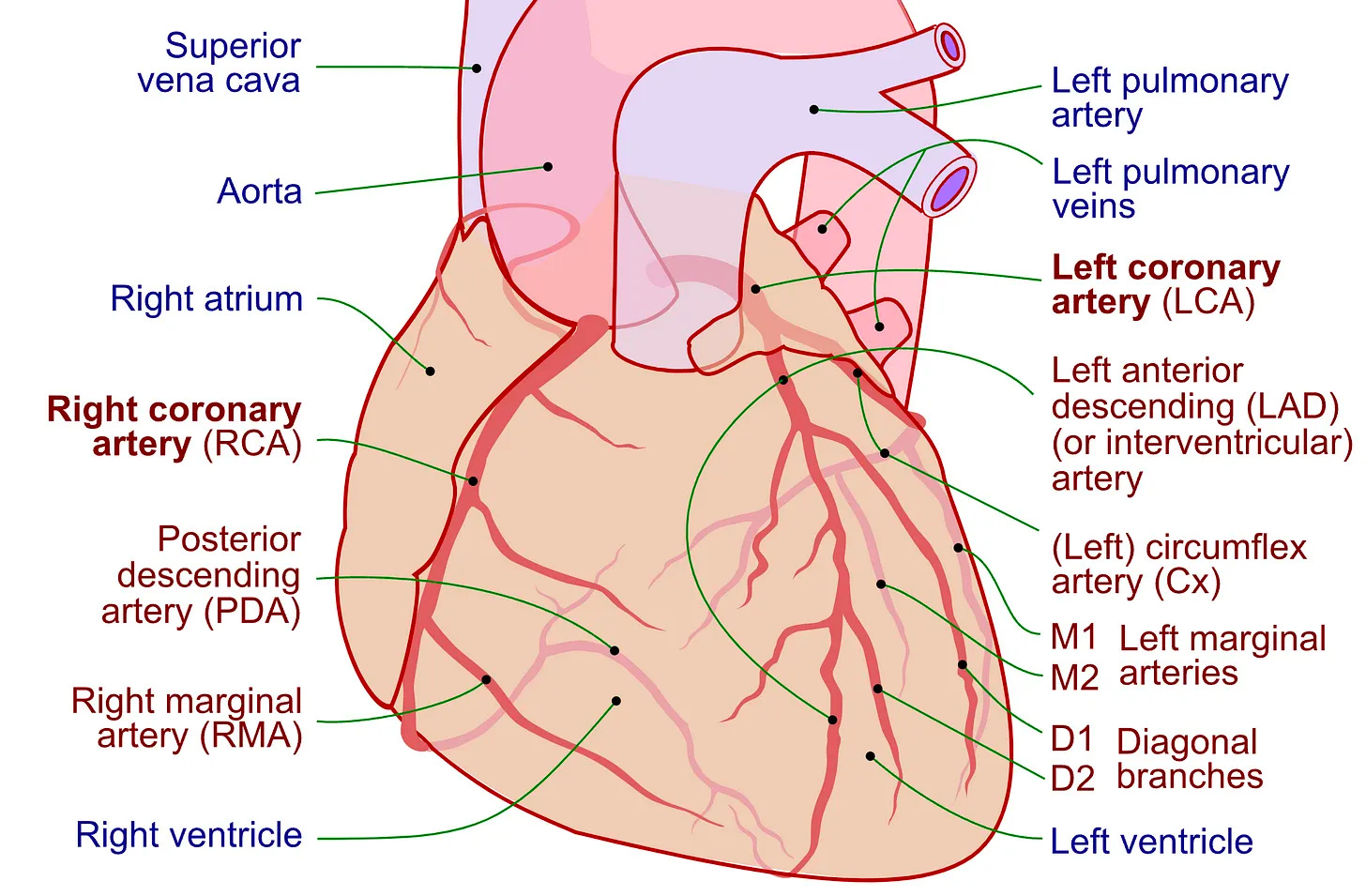
You can see that the right coronary artery (RCA) supplies the structures mentioned earlier in the following order, from proximal (i.e. from its origin above the right cusp of the aortic valve) to distal (i.e. its branch called the posterior descending artery):
SA node → Right Ventricle → AV node → Inferior wall of the Left Ventricle
Therefore, the more proximal the occlusion is, the more of these structures will be affected.
As the inferior wall of the left ventricle is the last area perfused by the RCA, it is the most commonly affected. Ischaemia of this area can be identified with a standard 12-lead transthoracic ECG, seen as an inferior STEMI (in cases of complete occlusion).
Question 3: Which lead should be used to check for ischaemia in the structure which is the right answer for Question 1?
As the right answer for question 1 is the Right Ventricle, the correct answer for question 3 is V4R. And no, placing V1 between the eyebrows is not the answer (… I think).
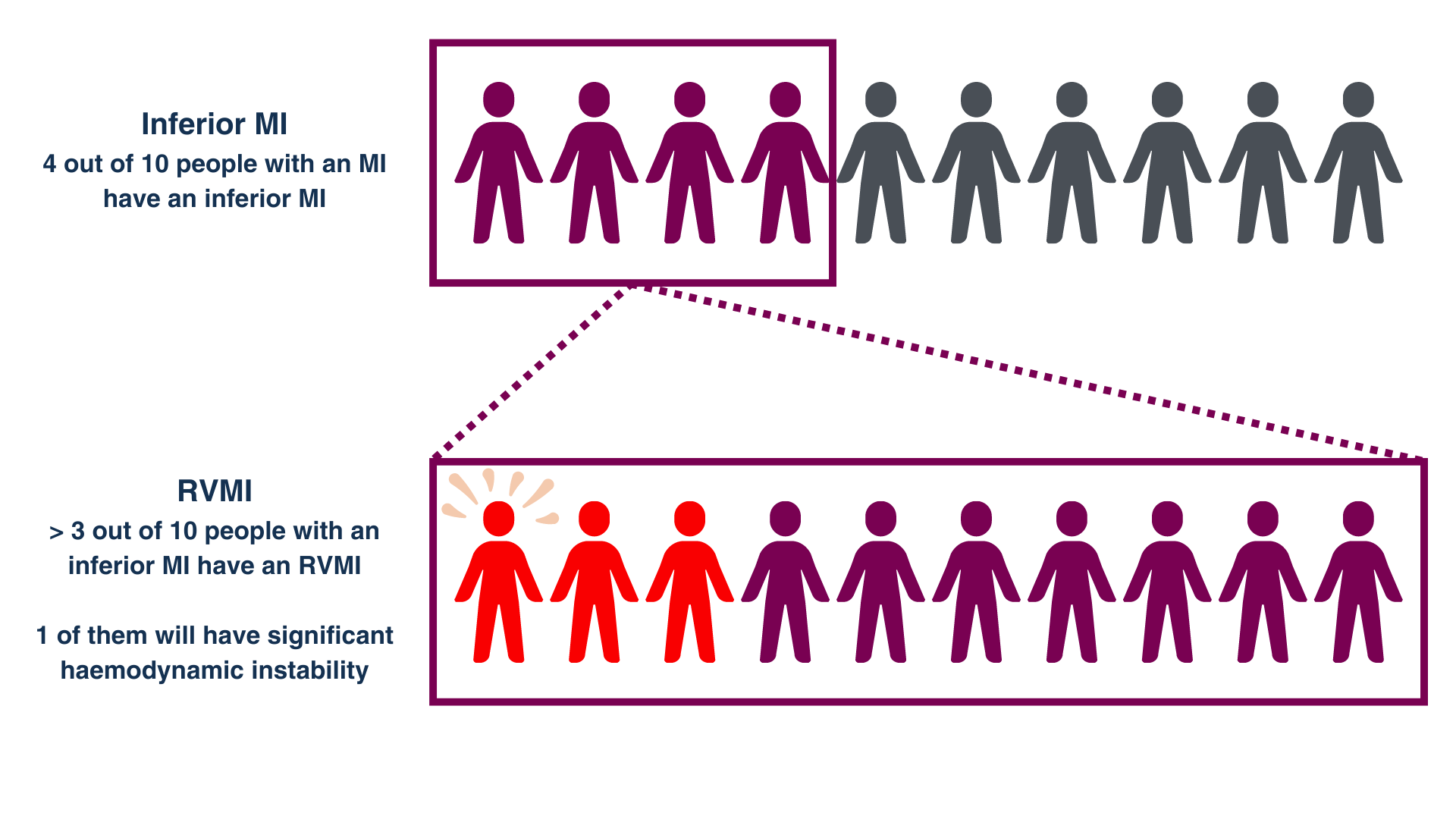
When you see an inferior STEMI, there is a 30-50% chance that the RV is also undergoing ischaemia.
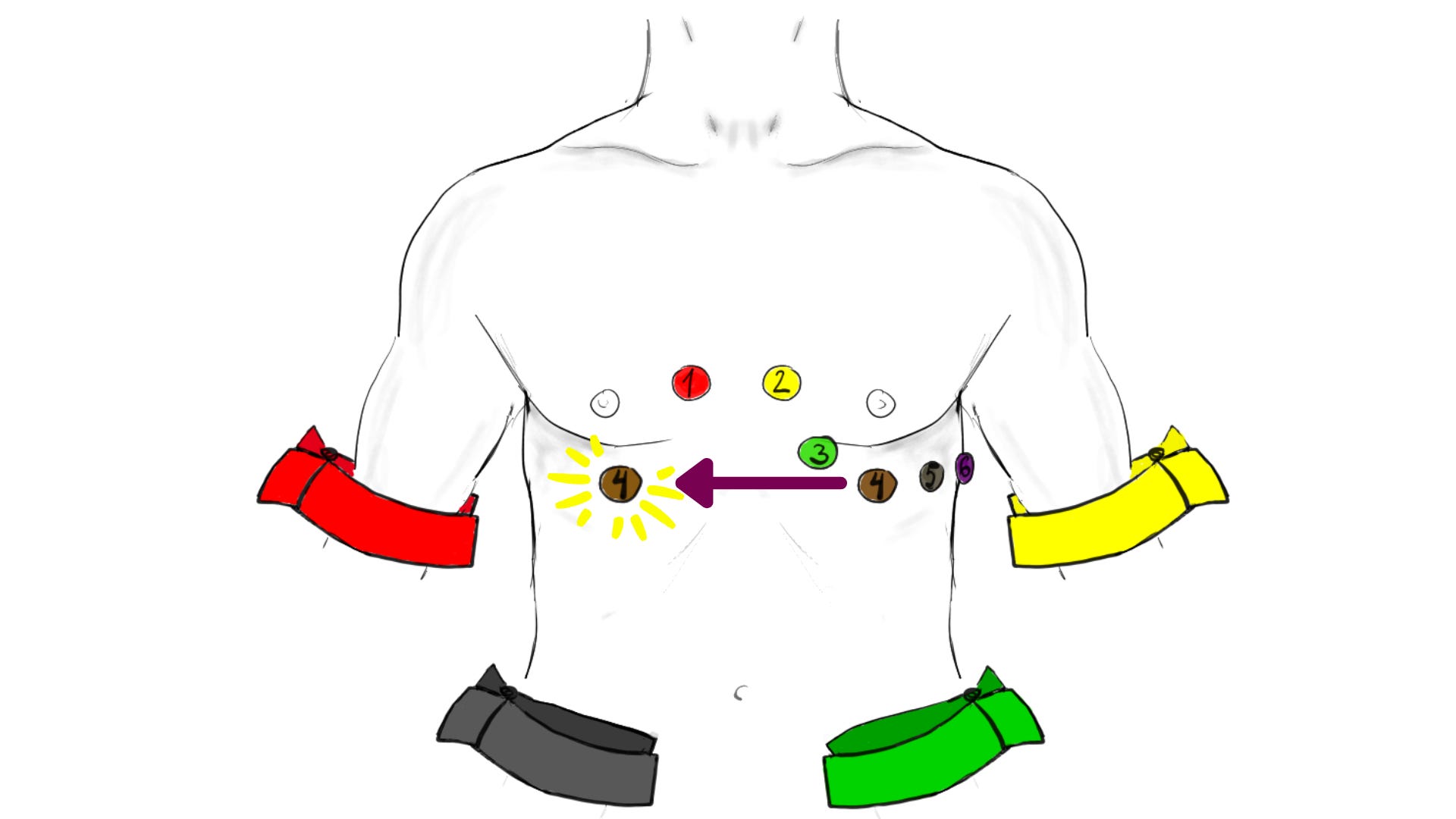
In order to confirm RV ischaemia, you will need to use the right precordial leads (V3R-V6R). The most useful is V4R.
Where do you place V4R? You would place it in the same location as V4 but on the right side of the body. Specifically, it should be placed in the 5th intercostal space on the right side of the body, in the mid-clavicular line (as shown in the picture below).2 The same logic applies to V3R, V5R, and V6R.
If there is suspicion of RV ischaemia, the most accurate way to diagnose it is to perform a right-sided ECG.
An ST elevation of greater than 1 mm in V4R has:
sensitivity of 100%
specificity of 87%
predictive accuracy of 92%
for RV ischaemia.
Why knowing about Right Ventricular Myocardial Infarction (RVMI) is important
1) It’s common - and we commonly miss it.
More than 30% of people with an inferior MI also have RV ischaemia. However, the conventional method for recording ECGs primarily focuses on the left ventricle and is not effective in identifying RV ischaemia or infarction.
2) Patients with RVMI are more likely to die in the hospital than those with isolated LVMI.
Although the long-term prognosis after treatment and resolution of an RVMI is similar to that of an LVMI, the short-term prognosis is worse. This is likely due to the complications associated with RVMIs.
3) RV dysfunction creates a preload-dependent heart (i.e. the heart needs its preload), and we commonly give drugs as part of MI treatment that reduce preload!
Acute RV dysfunction can arise from an RVMI. 10% of the patients with left ventricular inferior wall MIs have significant haemodynamic instability attributed to RV dysfunction.
Preload is crucial for the heart at this point: a drop in preload can have dramatic effects on the patient. This is why nitrates (which cause vasodilation and can reduce preload as well as afterload) may be harmful in these patients. Nitrates! Drugs which have a central role in the treatment of MIs!
So, if you see this…
If you see the following ECG3, it’s worth checking V3R-V6R, especially V4R.
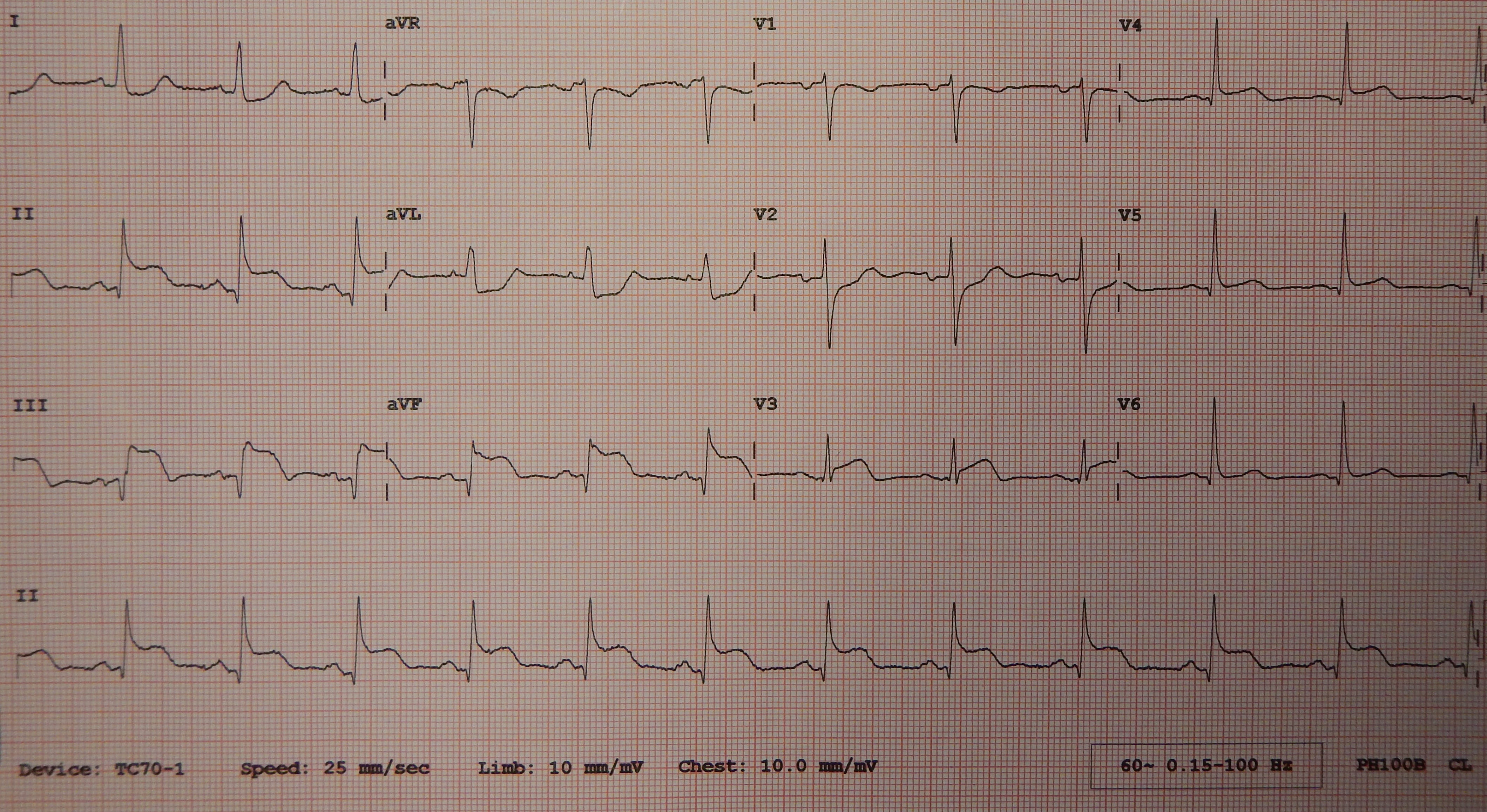
Here’s a challenge for those who want to take their ECG learning one step further:
There are two more findings here that increase even further the suspicion of RVMI. Do you know what those findings are? Write in the comment section below if you have any ideas, and keep an eye on Substack Notes, as I will post the answer there in the coming days.
Summary
The Right Ventricle (RV) is most commonly perfused by the Right Coronary Artery (RCA).
Inferior STEMI is most commonly associated with RCA occlusion.
If you see an inferior STEMI, check the right precordial leads, especially V4R.
Right Ventricular Myocardial Infarction (RVMI) is not rare, but often missed.
Patients with RVMI are more likely to die in the hospital than those with isolated LVMI.
RV dysfunction creates a preload-dependent heart, and certain drugs used in MI treatment that reduce preload can be harmful.
Feedback - Your opinion is crucial!
Your thoughts and experiences are invaluable to this community. By sharing them, you can directly shape the content of this newsletter, making it more relevant and valuable to your studies and interests.
So, please take a moment to share your thoughts. And if you found this post helpful, consider sharing it with your peers.
Together, we can make this a valuable resource for everyone!
What improvements would you recommend for this newsletter? What would you like to see more of in the publication?
If you answered yes to the first question, please take a moment to share the Squiggly Lines newsletter! This will help grow our community of enthusiastic learners!
Thank you for your time and feedback!
References
Jeffers JL, Boyd KL, Parks LJ. Right Ventricular Myocardial Infarction. [Updated 2022 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431048/
Lilly, L. S. (2021). Pathophysiology of Heart Disease (7th ed.). Wolters Kluwer.
Coronary.pdf: Patrick J. Lynch, medical illustratorderivative work: Fred the Oysteradaption and further labeling: Mikael Häggström, M.D. Author info - Reusing images- Conflicts of interest: NoneMikael Häggström, M.D., CC BY-SA 3.0 https://creativecommons.org/licenses/by-sa/3.0, via Wikimedia Commons
Baklazan99, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
This image has been amended to show the placement of V4R. It is licenced under the same licence as the original image (Creative Commons Attribution-Share Alike 4.0 International).
James Heilman, MD, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons