
The jumping heart | UKMLA challenge #1
A UKMLA-focused ECG challenge about a common cause of palpitations.

The case
A 55 year old woman has intermittent palpitations for 2 weeks. She describes brief episodes of her heart “suddenly jumping” a few times a day, mostly at rest.
She has hypertension managed with amlodipine and smokes 10 cigarettes a day.
Her pulse is 74 bpm and BP 153/94 mmHg. Heart sounds are normal.
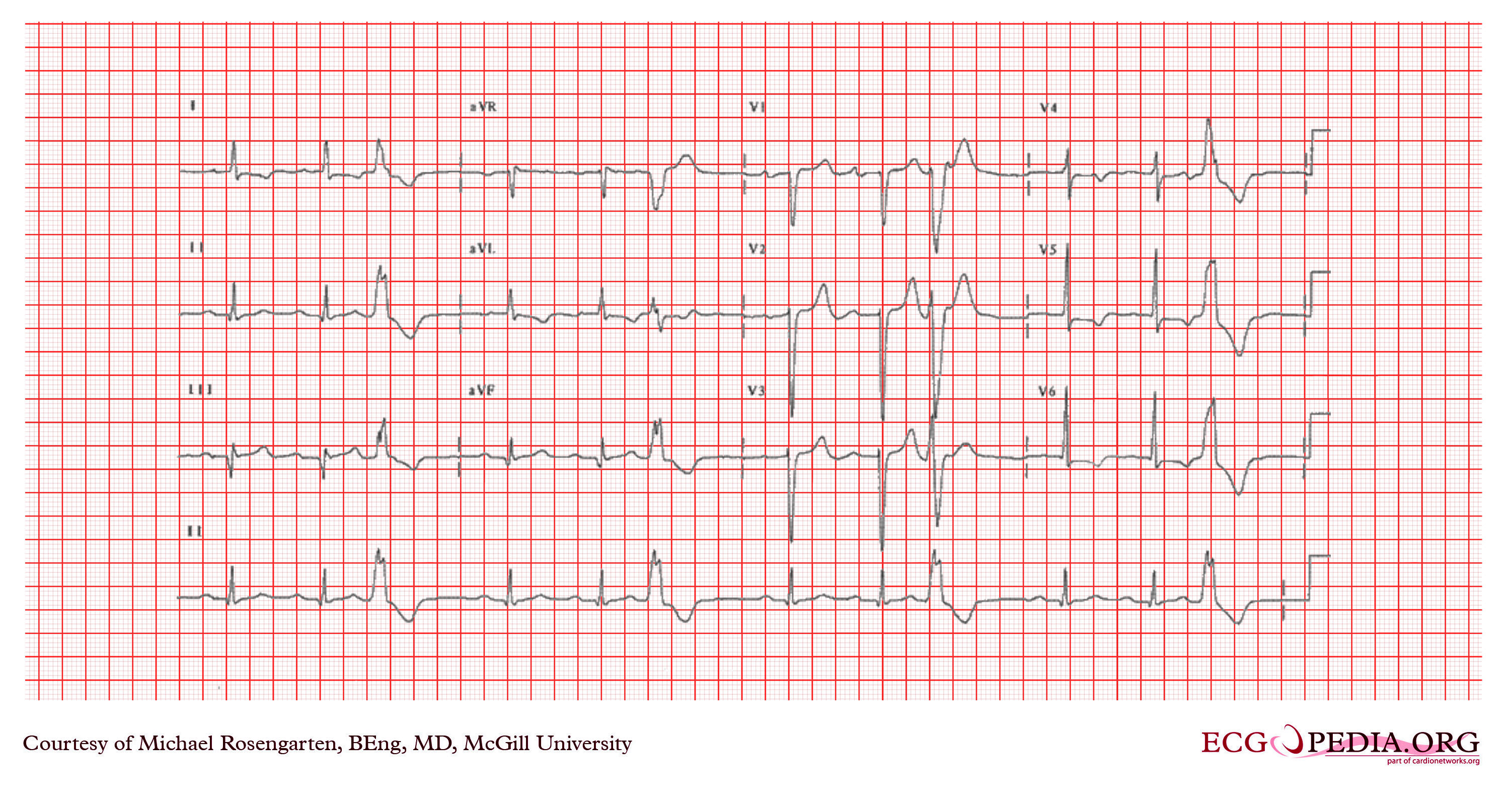
A 12-lead ECG is performed.
ECG systematic analysis
Assumed paper speed: 25 mm/s and voltage: 10 mm/mV (standard).
This ECG shows the following:
Rhythm: Sinus rhythm with ventricular trigeminy. Every third beat is a premature ventricular complex (four PVCs visible across the recording), each followed by a compensatory pause (see correct answer section below).
P waves: ~72 bpm, normal axis (positive in lead II, negative in aVR).
PR interval: 240 ms (prolonged; 1st degree AV block).
QRS complex:
Rate: ~80 bpm (including the PVCs).
Duration: Narrow in sinus beats (less than 120 ms); ~160 ms for the PVCs.
Axis: Normal in both the sinus beats and the PVCs.
Morphology: Pathological Q waves in leads II, III, and aVF (sinus beats). The PVCs are monomorphic (same morphology) with LBBB morphology and appropriate discordance.1
QT interval: 394 ms (QTcB - Bazett’s formula).
ST segment: 0.5–1 mm ST depression in leads I, V5, and V6 (sinus beats). The PVCs show expected repolarisation abnormalities (appropriate discordance).
T waves: T wave inversion in leads I, aVL, V4–V6.
Overall, this 12-lead ECG shows sinus rhythm with ventricular trigeminy and 1st degree AV block. Precordial voltage criteria for left ventricular hypertrophy are met (S in V2 + R in V6 = 37 mm, threshold > 35 mm). The lateral ST depression and T wave inversion are consistent with LVH with a strain pattern. Pathological Q waves are present in the inferior leads.
Correct answer
Premature ventricular complexes
Premature ventricular complexes (PVCs) arise from an ectopic focus somewhere in the ventricular myocardium that fires before the next sinus beat is due. They are found in up to 75% of healthy individuals on 24-hour Holter monitoring, but are more prevalent in patients with risk factors such as hypertension and smoking (both present here), which increase adrenergic drive and myocardial irritability.
On this ECG, the PVCs occur in a trigeminy pattern: every third beat is a PVC. They are monomorphic (identical in shape), which tells you they all originate from the same ectopic focus. If the PVCs had different morphologies (polymorphic), that would suggest multiple foci and warrant closer attention. This regular recurrence with a consistent coupling interval suggests a stable ectopic focus. You may also encounter bigeminy (every second beat) or quadrigeminy (every fourth beat).
You might also encounter two consecutive premature beats, known as couplets. Three or more consecutive PVCs at a rate exceeding 100 beats per minute is defined as ventricular tachycardia.
Every feature of these premature complexes can be derived from a single fact: the impulse originates in the ventricle:
No preceding P wave (and therefore no PR interval) because the impulse didn’t start in the atria.
Wide QRS (>120 ms) because the impulse doesn’t enter the His-Purkinje system at its normal entry point. Instead, it conducts via cell-to-cell transmission through the ventricular myocardium, which has a much slower conduction velocity. This is why any ventricular-origin beat (PVCs, VT, ventricular paced rhythms) produces a broad QRS.
Abnormal ST segment and T wave because the abnormal depolarisation pathway alters repolarisation too. The ST-T changes are directed opposite to the main QRS deflection. This is expected, called appropriate discordance, and does not indicate ischaemia.
Compensatory pause. The interval spanning the PVC equals exactly two normal RR intervals, because the SA node keeps firing on schedule and is never reset by the PVC. For why this happens (and why PACs behave differently).
See the article below for more context on premature complexes and the compensatory pause.

Noteworthy findings
The ECG also shows findings unrelated to the palpitations but consistent with the clinical picture. The precordial voltage criteria for LVH are met (S in V2 + R in V6 = 37 mm, exceeding the 35 mm threshold), and the lateral ST depression with T wave inversion represents a strain pattern. This is not ischaemia: there is no chest pain, and the ST-T changes follow the expected distribution for LV strain (lateral leads, discordant to the tall QRS voltages). The BP of 153/94 mmHg despite amlodipine tells you her hypertension is not well controlled, and longstanding poorly controlled hypertension is the most common cause of LVH.
The 1st degree AV block and inferior Q waves (possible inferior wall scar from an old myocardial infarction) are incidental findings that a systematic read-through would pick up, even though they don’t change the answer to this question.
Incorrect options
Atrial fibrillation. AF is a sustained rhythm that produces an irregularly irregular pattern with absent P waves throughout the entire recording. This ECG shows regular sinus rhythm interrupted by discrete extra beats. AF cannot produce isolated broad-complex beats interspersed in an otherwise normal sinus rhythm.
Premature atrial complexes. PACs originate above the ventricles and conduct through the His-Purkinje system normally, producing a narrow QRS, the same width as the sinus beats. Aberrant conduction can occasionally widen the QRS of a PAC, but a PAC is still preceded by a premature P wave (often buried in the preceding T wave, distorting its shape). The broad QRS complexes with no preceding P waves on this ECG point to a ventricular, not atrial, origin.
Premature junctional complexes. PJCs originate from the AV junction and, like PACs, conduct through the His-Purkinje system to produce a narrow QRS (again, unless there is aberrant conduction). They typically have no preceding P wave, or a retrograde P wave just before or after the QRS that is negative in the inferior leads. The key distinguishing feature here is QRS width: PJCs are narrow because they use the normal conduction pathway. These beats are broad. That rules out a junctional origin.
Ventricular tachycardia. VT is three or more consecutive ventricular beats at a rate above 100 bpm. Although this ECG has multiple PVCs, they are not consecutive.
When do PVCs actually matter?
Most isolated PVCs need nothing more than reassurance and lifestyle modification: stop smoking, reduce caffeine, manage stress. But they are not always innocent. The 2022 ESC guidelines on ventricular arrhythmias flag two thresholds:
PVC burden ≥10% on Holter monitoring with unexplained reduced ejection fraction → suspect PVC-induced cardiomyopathy.
PVC burden >20% even in asymptomatic patients without established cardiomyopathy → catheter ablation may be considered.
The management ladder: lifestyle modification → beta-blockers or non-dihydropyridine calcium channel blockers → catheter ablation.
For this patient, with infrequent symptomatic PVCs and no symptoms of haemodynamic compromise, the answer would be reassurance, lifestyle advice, and a low threshold for Holter monitoring if symptoms persist to assess the PVC burden.
Summary
How to identify a PVC on a 12-lead ECG:
It’s premature. The beat arrives before the next expected sinus beat. That makes it an ectopic, not an escape beat.
The QRS is wide on a baseline with no conduction disease. The impulse didn’t use the His-Purkinje system, so it conducted slowly through the ventricular myocardium. Wide QRS = ventricular origin (or aberrant conduction or baseline conduction disease, which is not the case here).
There is no preceding P wave. The impulse didn’t start in the atria or the SA node. Combined with a wide QRS, this points to a ventricular origin.
Compensatory pause. The SA node is not reset, so the next sinus beat arrives on schedule. The interval spanning the PVC equals exactly two normal RR intervals.
References
Sattar Y, Hashmi MF. Premature Ventricular Complex. [Updated 2025 Feb 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547713/
Zeppenfeld K, Tfelt-Hansen J, de Riva M, et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. European Heart Journal. 2022;43(40):3997–4126. DOI: 10.1093/eurheartj/ehac262
Surawicz B, Knilans TK. Chou’s Electrocardiography in Clinical Practice. 6th ed. Saunders Elsevier; 2008.
Appropriate discordance means the ST segment and T wave point in the opposite direction to the main QRS deflection (positive QRS → ST depression and T wave inversion; negative QRS → ST elevation and upright T wave). Whenever the ventricle depolarises with an LBBB morphology (LBBB, ventricular paced rhythm, PVC), this is an expected finding. It would be abnormal not to have it.
The Sgarbossa criteria use this principle to diagnose myocardial infarction in the presence of LBBB (see article below).
