
Common and irregular | UKMLA challenge #2
A UKMLA-focused challenge: how well do you know the management of the commonest arrhythmia?

A 71 year old man has palpitations for several weeks. His only medical history is diet-controlled type 2 diabetes mellitus.
His pulse is 88 bpm and irregularly irregular. BP is 128/76 mmHg. Weight is 78 kg.
Investigations:
Creatinine 92 μmol/L (60–110)
eGFR 77 mL/min/1.73 m² (>60)
A 12-lead ECG is performed (assume paper speed: 25 mm/s and voltage: 10 mm/mV (standard))

A repeat ECG performed an hour later shows sinus rhythm.
ECG systematic analysis
Assumed paper speed: 25 mm/s and voltage: 10 mm/mV (standard).
This ECG shows the following:
Rhythm: Irregularly irregular with no discernible P waves.
P waves: Absent.
PR interval: Not applicable (no organised atrial depolarisation).
QRS complex:
Rate: ~90 bpm.
Duration: Narrow (less than 120 ms).
Axis: Normal (positive in leads I and II).
Morphology: Normal. No pathological Q waves. No bundle branch block pattern.
QT interval: 348 ms (QTcB 425 ms, Bazett’s formula). Normal.
ST segment: No significant ST elevation or depression.
T waves: Normal morphology and direction.
Overall, this 12-lead ECG shows atrial fibrillation with a controlled ventricular response (~90 bpm).
Correct answer
Start apixaban 5 mg twice daily
Every ECG feature of AF can be derived from the fact that the atria have lost all organised electrical activity. Instead of the SA node firing in an orderly sequence, multiple re-entrant wavelets and focal triggers depolarise the atria chaotically at 350 to 600 impulses per minute. The two defining features follow directly:
No P waves because there is no single, coordinated atrial depolarisation to produce one. The organised wave that normally sweeps from the SA node to the AV node has been replaced by electrical chaos. In some patients, the chaotic atrial activity produces visible fibrillatory deflections (f waves) on the baseline. These can range from barely perceptible to coarse undulations that superficially resemble the sawtooth pattern of atrial flutter. The presence or absence of visible f waves does not change the diagnosis (the absence of P waves is the important bit).
Irregularly irregular rhythm because the AV node is bombarded by hundreds of impulses per second and conducts them variably. Some impulses arrive during the refractory period and are blocked; others get through. The result is unpredictable variation in the R-R intervals. The QRS is typically narrow because ventricular conduction via the His-Purkinje system is unchanged, but AF can coexist with bundle branch block, pre-excitation, or other causes of QRS widening. A wide QRS does not rule out AF.
Now the management question. Someone may instinctively want to “fix the rhythm” when they see AF, but the most dangerous thing about AF is not the arrhythmia itself. It is the thromboembolism risk. In AF, the atria are not contracting effectively. Blood stagnates (particularly in the left atrial appendage), leading to clot formation that can cause embolic events, such as stroke.
The tool for this is the CHA₂DS₂-VA score:1
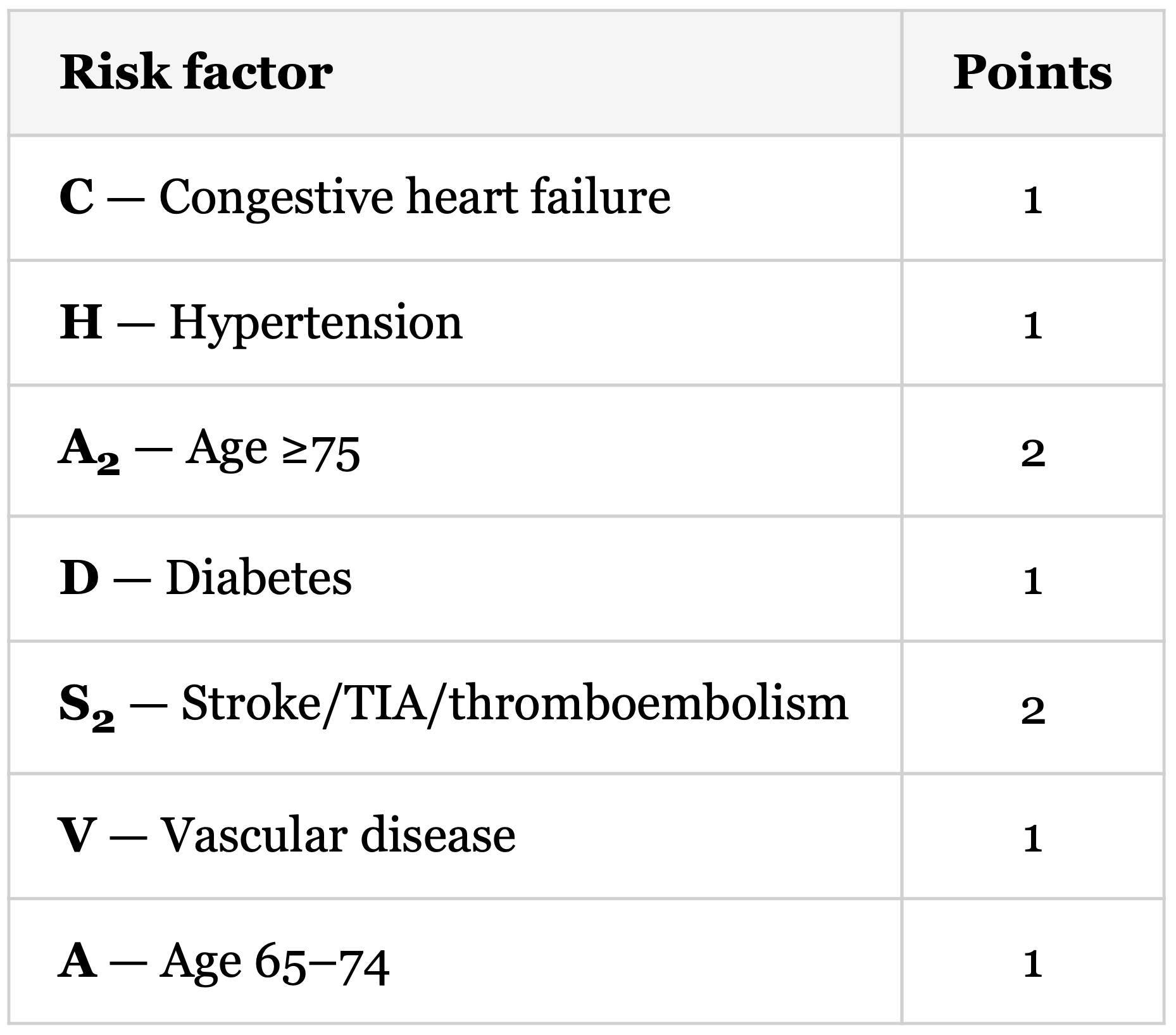
A CHA₂DS₂-VA of 2 meets the threshold for anticoagulation. The 2024 ESC guidelines recommend anticoagulation for patients with a CHA₂DS₂-VA score of ≥ 2 (Class I) and consider it for a score of 1 (Class IIa). This patient scores 1 for age and 1 for diabetes, so the total is 2.
The repeat ECG showing sinus rhythm an hour later tells you this is paroxysmal AF. The 2024 ESC guidelines classify AF into five patterns:
first diagnosed (not previously diagnosed, regardless of symptom status, pattern, or duration)
paroxysmal (terminates spontaneously within 7 days, or with the assistance of an intervention)
persistent (not self-terminating; many intervention trials have used 7 days as a cutoff). Long-standing persistent AF is continuous AF of at least 12 months’ duration where rhythm control is still a treatment option, distinguishing it from permanent AF.
permanent (no further attempts at restoring sinus rhythm are planned, after a shared decision between patient and physician).
This patient’s AF terminated spontaneously within hours, placing it in the paroxysmal category. The critical teaching point: the anticoagulation decision is the same regardless of AF pattern. Whether AF is paroxysmal, persistent, or permanent, the decision to anticoagulate is based on the patient’s CHA₂DS₂-VA score, not on how often AF occurs or how long each episode lasts. A patient whose AF comes and goes is managed the same way as one whose AF is constant.
Direct oral anticoagulants (DOACs) are first-line over warfarin for non-valvular AF. Apixaban, rivaroxaban, edoxaban, and dabigatran are all options. Warfarin is reserved for patients with moderate-to-severe mitral stenosis or mechanical heart valves, where DOACs are contraindicated.2
Noteworthy findings
The ventricular rate of ~88 bpm tells you this is AF with a controlled ventricular response. The 2024 ESC guidelines recommend a lenient rate-control target of less than 110 bpm at rest as an acceptable initial approach, so there is no urgency to start rate control. If he were tachycardic during episodes (say, 140-150 bpm), rate control would become more pressing.
The absence of LVH, ischaemic changes, or conduction abnormalities on this ECG is also relevant. It suggests AF in a heart without gross structural or electrical abnormalities (though you wouldn’t rely solely on an ECG), which influences the long-term rhythm-control strategy (e.g. flecainide if the heart is structurally normal).
Incorrect options
Reassurance. The repeat ECG shows sinus rhythm, but that does not mean the problem has resolved. This patient has documented AF and a CHA₂DS₂-VA of 2. The fact that the arrhythmia self-terminated does not reduce the need for anticoagulation.
Start amiodarone 200 mg three times daily. Amiodarone is a rhythm-control drug. Rhythm control may be considered later, but the immediate priority is stroke prevention. Amiodarone is also not first-line for rhythm control in paroxysmal AF with a structurally normal heart. Flecainide would be tried first. Amiodarone is reserved for patients with structural heart disease or when other agents have failed, and it carries significant long-term toxicity (thyroid, liver, lung, skin).
Start aspirin 75 mg once daily. Aspirin is an antiplatelet, not an anticoagulant. It inhibits platelet aggregation, which is relevant in arterial thrombosis driven by platelet-rich clots (for example, in acute coronary syndromes). The thrombi that form in AF are predominantly fibrin-rich, driven by blood stasis and coagulation cascade activation in the low-flow environment of the left atrial appendage. Anticoagulants target the coagulation cascade that produces these clots; antiplatelets do not.
Start bisoprolol 2.5 mg once daily. Bisoprolol is a rate-control drug. Rate control may well be needed if he has symptomatic episodes with a rapid ventricular rate, but the question asks for the most appropriate initial management. With a CHA₂DS₂-VA of 2, the first step is anticoagulation. His current ventricular rate is 88 bpm, which is already controlled (less than 110 bpm).
Summary
Key aspects of managing a new diagnosis of AF:
Recognise AF on the ECG. Irregularly irregular rhythm + absent P waves.
Classify. First diagnosed, paroxysmal (self-terminating or terminated by intervention within 7 days), persistent (not self-terminating; 7 days used as a conventional cutoff), long-standing persistent (≥12 months, rhythm control still considered), or permanent (no further rhythm control planned, shared decision).
Assess stroke risk. Use CHA₂DS₂-VA. The anticoagulation decision is the same regardless of AF pattern. 2024 ESC guidelines: ≥2 (Class I), ≥1 (Class IIa). DOAC is first-line for non-valvular AF.
Address symptoms. Rate control (beta-blockers, rate-limiting calcium channel blockers, or digoxin) for symptom management. Consider rhythm control if symptoms persist.
Manage comorbidities. Obesity, hypertension, sleep apnoea, alcohol, and other modifiable risk factors all contribute to AF burden.
Check out the following articles:


References
Isabelle C Van Gelder, Michiel Rienstra, Karina V Bunting, Ruben Casado-Arroyo, Valeria Caso, Harry J G M Crijns, Tom J R De Potter, Jeremy Dwight, Luigina Guasti, Thorsten Hanke, Tiny Jaarsma, Maddalena Lettino, Maja-Lisa Løchen, R Thomas Lumbers, Bart Maesen, Inge Mølgaard, Giuseppe M C Rosano, Prashanthan Sanders, Renate B Schnabel, Piotr Suwalski, Emma Svennberg, Juan Tamargo, Otilia Tica, Vassil Traykov, Stylianos Tzeis, Dipak Kotecha, ESC Scientific Document Group , 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): Developed by the task force for the management of atrial fibrillation of the European Society of Cardiology (ESC), with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Endorsed by the European Stroke Organisation (ESO), European Heart Journal, Volume 45, Issue 36, 21 September 2024, Pages 3314–3414, https://doi.org/10.1093/eurheartj/ehae176
National Institute for Health and Care Excellence. Atrial fibrillation: diagnosis and management. NICE guideline NG196. 2021 (last updated June 2021). Available from: https://www.nice.org.uk/guidance/ng196
The 2024 ESC guidelines use CHA₂DS₂-VA, which drops the sex category from the older CHA₂DS₂-VASc score. NICE NG196 still uses CHA₂DS₂-VASc: offer anticoagulation at a score of ≥2 (1.6.3), consider it for men with a score of 1 (1.6.4). For this patient, the score is 2 under both systems.
Apixaban dose reduction to 2.5 mg twice daily is required when at least two of the following three criteria are met: age ≥80 years, body weight ≤60 kg, serum creatinine ≥133 μmol/L. This patient meets none (age 71, weight 78 kg, creatinine 92 μmol/L).