


AV block, but what kind? | ECG challenge #5
This ECG shows an inferior STEMI with an AV conduction abnormality. Can you identify the type?

Clinical case
A 68-year-old man presents to the emergency department with sudden onset central chest pain radiating to his left arm, which started 1 h ago while he was gardening.
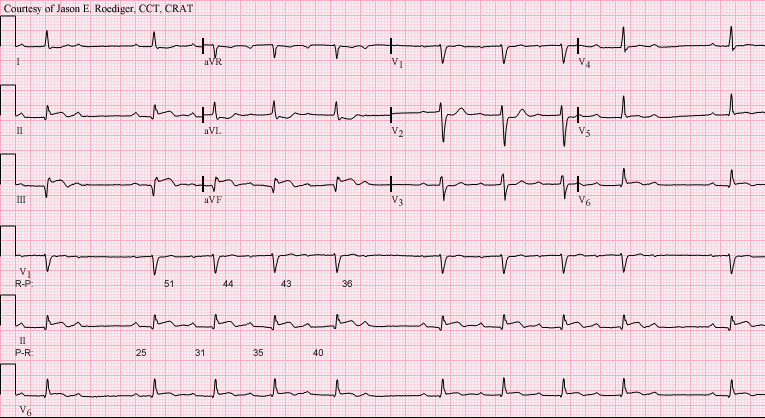
A 12-lead ECG is performed. See image below.
ECG systematic analysis
Assumed paper speed: 25 mm/s and Voltage: 10 mm/mV (standard).
This ECG shows the following:
Rhythm: Sinus rhythm with a 2nd-degree AV block Mobitz I (Wenckebach), with a 5:4 conduction
P waves: ~80 bpm, normal axis
PR interval: Starts at 240 ms and progressively lengthens until a P wave is not conducted
QRS complex:
Rate: ~60 bpm (slower than the atrial rate because one out of five atrial waves is not conducted).
Duration: Normal (less than 120 msec)
Axis: Positive in leads I and II; therefore, the QRS axis is normal.
Morphology: Pathological Q waves in leads II, III and aVF
Normal
QT interval: 400 ms (QTcB)
ST Segment: ST elevation in leads II, III, aVF, and V6. Reciprocal ST depression in leads I and aVL, with additional depression in lead V2.
T waves: Biphasic T waves in leads III and aVF
Overall, this 12-lead ECG shows a sinus rhythm with a 2nd-degree AV block type I (Wenckebach), with a 5:4 conduction. It also shows an inferior STEMI with possible posterior wall involvement as well (in view of the ST depression in lead V2, even though there’s no tall R wave in V2).
Correct answer
The correct answer is 2nd degree AV block Mobitz I.
This diagnosis is based on the ECG findings, which show a progressive prolongation of the PR interval with each successive beat until a P wave is not followed by a QRS complex—a dropped beat. After this non-conducted P wave, the cycle repeats.
This pattern is known as the Wenckebach phenomenon, a hallmark of Mobitz type I block, and it is due to progressive prolongation of the refractory period of the AV node. When an atrial impulse passes through the AV node during the relative refractory period, it conducts more slowly, prolonging the PR interval. Eventually, an impulse arrives when the AV node is in its absolute refractory period and will not be conducted.
Mobitz type I (Wenckebach) block typically occurs at the level of the AV node and is often transient, especially in the context of acute myocardial infarction. It is less likely to progress to complete AV block compared to Mobitz type II.
The ECG in this case also demonstrates features of an inferior STEMI, which can be associated with transient AV nodal conduction abnormalities such as Mobitz type I block.
Regarding the incorrect options:
1st-degree AV block is characterised by a consistently prolonged PR interval with 1:1 AV conduction; there are no dropped beats.
3rd-degree AV block occurs when there is complete AV dissociation, meaning atrial and ventricular activity are independent.
Second-degree AV block Mobitz II shows intermittent dropped beats with a constant PR interval, unlike in this case, where the PR interval progressively lengthens.
Summary
When there’s intermittent AV conduction, this is a 2nd-degree AV block.
When this intermittent conduction is associated with a progressive prolongation of the PR interval, it’s a 2nd-degree AV block Mobitz I.

