
How to describe cardiac conduction like a pro
A guide to sounding very impressive when citing ECG findings in a cardiology referral.

You’re on the phone with the cardiology registrar. The ECG is in front of you, and for once, you actually know what you’re looking at. You’ve been waiting for this moment for years. You take a breath and begin.
“Thank you for taking my call. I have a 74-year-old gentleman with a background of ischaemic heart disease. His ECG shows evidence of advanced interatrial block, with a P wave duration of 130 milliseconds and biphasic in lead II. The PR interval is 220 milliseconds with 1-to-1 AV conduction, in keeping with first-degree AV block, and the QRS duration is 130 milliseconds with a morphology consistent with right bundle branch block...”
You pause. You can almost hear them nodding through the phone.
“What’s the ejection fraction?”
You stutter. “S... s... sorry?”
“What. Is. The. Ejection. Fraction?”
Maybe I’ll just impress my colleagues in orthopaedics then (spoiler: I tried, they didn’t care).
What is conduction on an ECG?
The ECG fundamentally records two things: time (the x-axis) and voltage (the y-axis). Everything else is derived from these two.
Duration: how long a wave or interval lasts on the x-axis.
Voltage: how tall or deep a deflection is on the y-axis.
Axis: the direction of the wavefront, derived from comparing voltages across leads.
Morphology: the shape of the waveform (the pattern of voltage changes over time).
Duration. Conduction is, at its core, how long the electrical impulse takes to travel through a region of the heart — a measurement of time, on the x-axis.

A wider P wave means slower atrial conduction.1 A longer PR interval means slower AV conduction. A wider QRS means slower ventricular conduction.
Duration is the primary axis, but conduction is also about whether the impulse gets through at all. Conduction abnormalities exist on a spectrum: the impulse can be delayed (slow but still conducted), intermittently blocked (some impulses get through, others don’t), or completely blocked (nothing gets through). First-degree AV block is a pure duration problem. Second-degree AV block is a pass/fail problem. Third-degree is total failure.
Duration is what you measure when conduction is slow. Missing waveforms are what you see when conduction fails.
Conduction abnormalities can also alter morphology, because they change the sequence of depolarisation. Bundle branch blocks widen the QRS and change its shape. WPW pre-excitation shortens the PR interval and adds a delta wave.
Intraatrial conduction
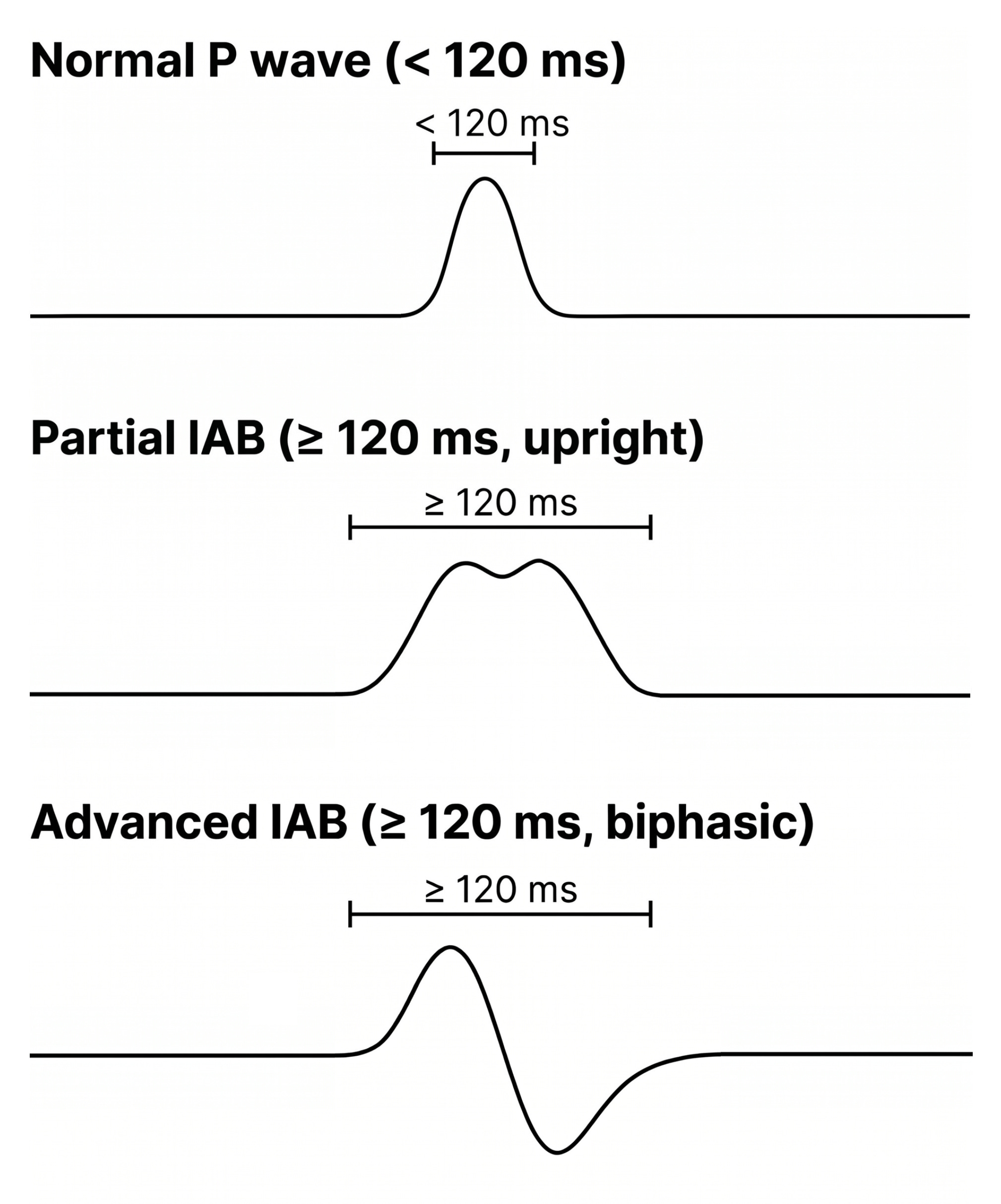
Intraatrial conduction is reflected by the P wave duration. Normal: < 120 ms (3 small squares).
The P wave represents the time for the electrical impulse to travel from the SA node through both atria. The SA node’s own depolarisation isn’t visible on the ECG: its tissue mass is too small to generate a measurable surface voltage. What you see is the wave it triggers in the much larger atrial myocardium, beginning a few milliseconds after the SA node fires. That wave starts with sinoatrial conduction (the impulse exiting the SA node into the surrounding atrial tissue), which is really the very first segment of intraatrial conduction. The Bachmann bundle then carries the impulse across the interatrial septum to the left atrium.
(More on atrial conduction abnormalities here.)
When intraatrial conduction is delayed (P wave ≥ 120 ms), this is classified as interatrial block: the impulse takes too long to reach the left atrium, usually because the Bachmann fibres are diseased or fibrotic [1].
Can intraatrial conduction be abnormally fast? Not in any clinically meaningful way. There is no recognised "intraatrial pre-excitation" on a standard ECG.
Atrioventricular conduction
Atrioventricular (AV) conduction is reflected by the PR interval. Normal: 120 to 200 ms (3 to 5 small squares).
The PR interval represents the time from the onset of atrial depolarisation to the onset of ventricular depolarisation. Most of this time is spent in the AV node, which is deliberately slow. Its cells fire via calcium channels (slower than the sodium channels used elsewhere) and couple loosely to their neighbours. The delay exists by design: it gives the atria time to finish contracting before the ventricles fire.
The AV node is the bottleneck, and it dominates the PR interval.
, first-degree AV block (PR > 200 ms), and pre-excitation WPW (PR < 120 ms with delta wave)")
Slow AV conduction (PR > 200 ms): this is first-degree AV block, which is not really a block at all. Every impulse still reaches the ventricles; it just takes longer [2]. When AV conduction fails rather than just delays, you get second- or third-degree block.
, second-degree Mobitz I (progressive PR then dropped beat), and third-degree (P and QRS dissociated)")
(More on AV blocks here.)
Fast AV conduction (PR < 120 ms): this is pre-excitation. An accessory pathway bypasses the AV node, allowing the impulse to reach the ventricles ahead of schedule. In Wolff-Parkinson-White (WPW) pattern (the most well known example of pre-excitation), you see a short PR, a delta wave, and a widened QRS [3].
(More on pre-excitation here.)
AV conduction is the only level where the language of medicine has names for being too slow and too fast.
Intraventricular conduction
Intraventricular conduction is reflected by the QRS duration. Normal: < 120 ms (3 small squares).
The QRS represents the time for the impulse to travel through both ventricles. Normally, this is fast: the His-Purkinje system uses sodium-mediated action potentials and is richly connected by gap junctions, giving it low electrical resistance and high conduction velocity [4]. Both ventricles depolarise near-simultaneously, keeping the QRS narrow.
When intraventricular conduction is delayed (QRS ≥ 120 ms), this is an intraventricular conduction delay (IVCD). If the broad QRS meets specific morphological criteria in V1 and V6, it is classified as RBBB or LBBB. If it doesn’t meet those criteria, it is called a non-specific IVCD.
, RBBB (rsR', qRS with broad S), and LBBB (rS, broad R)")
(More on bundle branch blocks here.)
There is also a subtler form of conduction abnormality here. Left fascicular blocks (left anterior and left posterior) alter the QRS axis without widening it beyond 120 ms. They represent conduction delay within one of the fascicles of the left bundle branch rather than the whole bundle [3].
What about abnormally fast intraventricular conduction? The QRS doesn’t get shorter than normal. The closest is WPW pre-excitation, where the accessory pathway widens the QRS rather than shortens it.
Summary
Back to the cardiology registrar. Your patient’s ECG shows: P wave 130 ms, PR 220 ms, QRS 130 ms with RBBB morphology. Where is the conduction abnormality?
All three tiers. Advanced interatrial block. First-degree AV block. Right bundle branch block. One ECG, three layers of conduction disease.
, PR interval (AV), and QRS (intraventricular) with normal durations and 'too slow' and 'too fast' diagnoses")
Just make sure you also check the ejection fraction.
References
Alexander B, Tse G, Martinez-Selles M, Baranchuk A. Atrial Conduction Disorders. Curr Cardiol Rev. 2021;17(1):68-73. doi: 10.2174/1573403X17666210112161524.
Ahmed I, Goyal A, Chhabra L. Atrioventricular Block. [Updated 2024 Feb 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459147/
Surawicz, B, Childers, R, Deal, B. et al. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part III: Intraventricular Conduction Disturbances. JACC. 2009 Mar, 53 (11) 976-981. https://doi.org/10.1016/j.jacc.2008.12.013
Lilly LS. Pathophysiology of Heart Disease: A Collaborative Project of Medical Students and Faculty (7th ed.). Wolters Kluwer; 2021.
Image credits
PR-interval triptych: Top: CardioNetworks: Drj, CC BY-SA 3.0. Middle: Adapted from Npatchett, CC BY-SA 4.0. Bottom: Adapted from CardioNetworks: Googletrans, CC BY-SA 3.0. All via Wikimedia Commons. Composite released under CC BY-SA 4.0.
AV block spectrum: All panels adapted from Npatchett, CC BY-SA 4.0, via Wikimedia Commons. Composite released under CC BY-SA 4.0.
QRS V1/V6 triptych: Bottom (LBBB) waveforms adapted from Andrewmeyerson, CC BY-SA 3.0, via Wikimedia Commons. Other panels public domain. Composite released under CC BY-SA 4.0.
Some sources distinguish interatrial conduction delay (slowed conduction across the Bachmann region, between the atria) from intra-atrial conduction delay (slowed conduction within an atrium itself, typically the left). The two are mechanistically distinct but produce the same wide upright P wave on the surface ECG. For simplicity, this article uses intraatrial conduction as the umbrella term and refers to interatrial block where the distinction matters. See the dedicated post linked above for the mechanism in detail.