


PR interval
Learn everything you need to know about identifying a normal PR interval.

Introductory quiz
Here are a few warm-up questions to get our brains going:
Intervals vs segments
When referring to "intervals" (like the PR and QT intervals) on an ECG, we want to know their duration only. If we wanted to know about morphology, we would be referring to the PR segment, not interval.
PR interval
The PR interval is the period from the beginning of the P wave until the beginning of the QRS complex (excluding the QRS complex). Therefore, the PR interval includes the P wave and the PR segment (the line connecting the P wave to the QRS complex), as seen in the picture below.

If the PR interval ends just before the QRS complex, why is it not called the PQ interval?
Indirect answer: Sometimes, it is referred to as the PQ interval (rarely).
Devil’s advocate answer: Sometimes, the QRS complex starts with an R wave, such as in lead V1.
Truthful-direct answer: I don't know…
The physiological representation of the PR interval is the depolarisation of the atria (P wave) AND the depolarisation of the AV junction (AV node and His bundle). In the following image, you can see the location of the AV junction in relation to the atria and the ventricles.
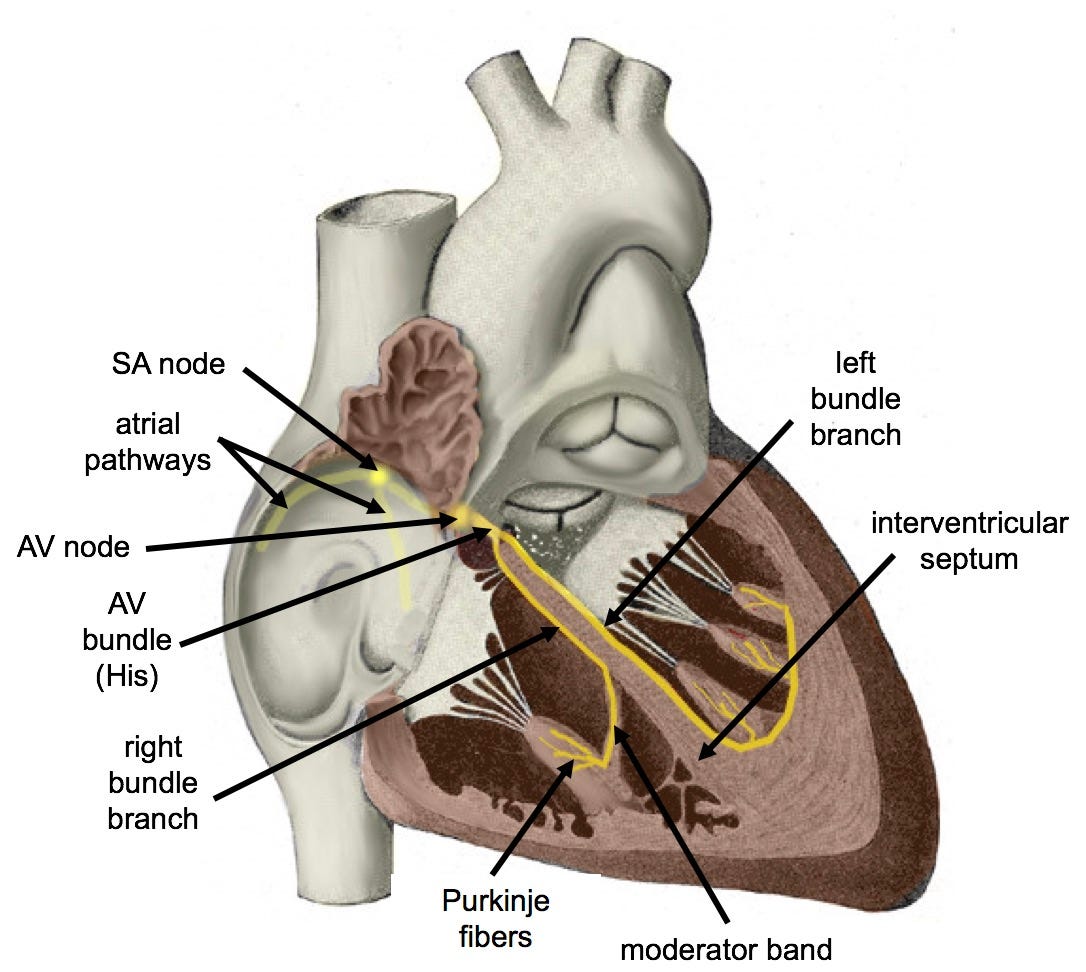
Also, in case you hadn’t noticed, the AV junction (similarly to the SA node) is completely silent on the transthoracic ECG (i.e. we don’t see any spikes recorded because of its depolarisation).
AV junction: the heart’s timekeeper
The AV junction is the reason why there’s a delay between atrial and ventricular depolarisation and contraction. This delay allows the ventricles to fill with the last volume of blood from the atria before contracting, which optimises cardiac output.
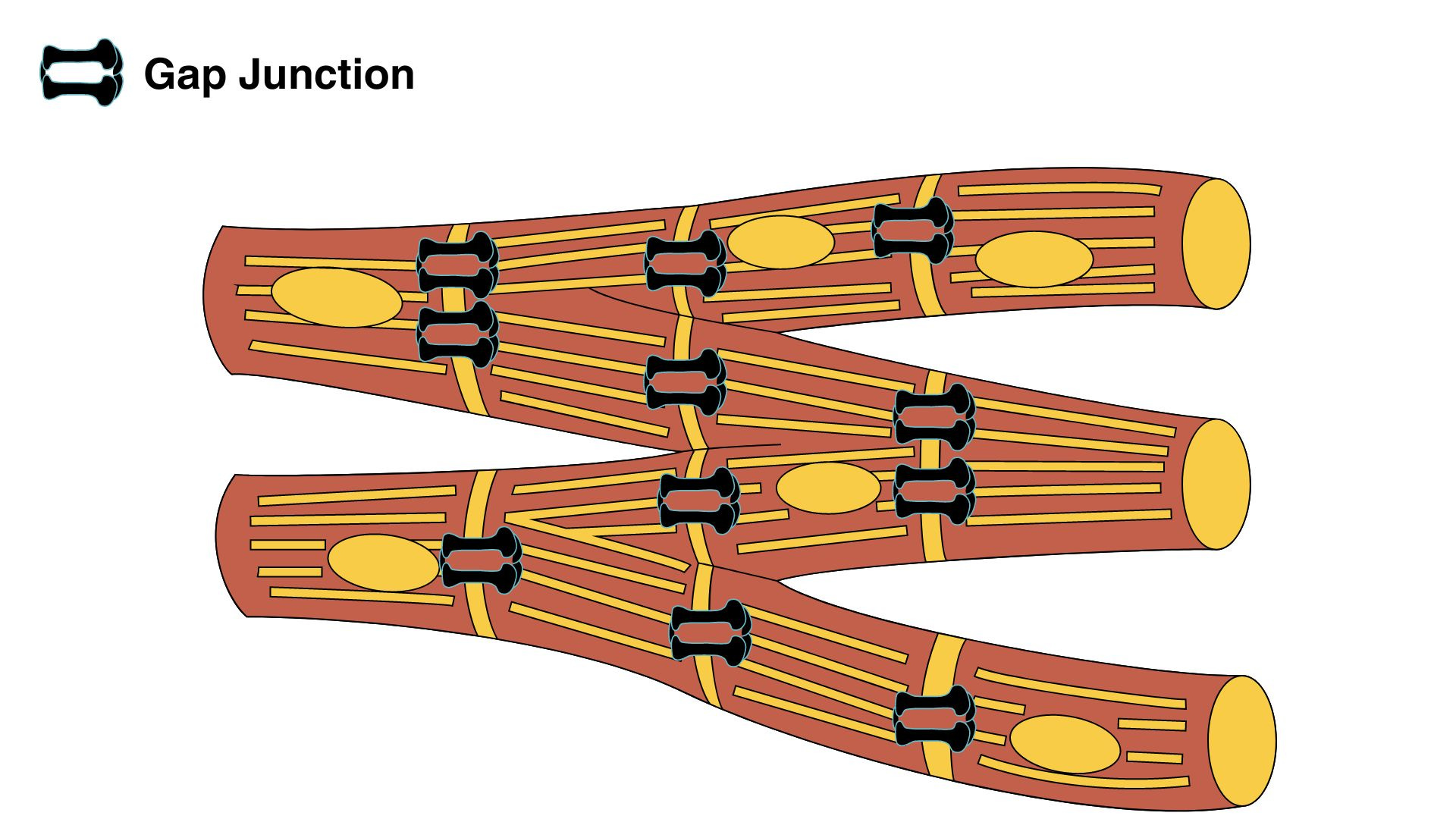
Slower conduction velocity in the AV junction
The answer is fewer gap junctions between the cells in the AV junction. Gap junctions are intercellular channels for ion transmission (i.e. for electrical current flow).
Imagine the gap junctions as doors allowing access to ions (i.e. electrical current) from one cardiac cell to the next. The fewer doors you have (increased resistance), the more difficult it becomes for ions to move (reduced current). This is governed by Ohm’s law, which states that current flow is directly proportional to the voltage across two points (in this case, across the cell membrane, also known as membrane potential) and inversely proportional to the resistance between them (the number of gap junctions).
I: current
V: voltage
R: resistance
The fewer gap junctions you have, the greater the resistance.
Answers to introductory quiz questions
1. What is the normal range for the PR interval (in adults)?
The normal PR interval in most adults is 120 - 200 msec.
Remember, this duration includes the duration of the P wave. You start measuring the PR interval from the start of the P wave.
2. "The length of the PR interval should always remain constant unless there is an abnormality present.”
This statement is false.
Firstly, the PR interval is not exactly the same in every lead and can vary slightly from lead to lead.
Secondly, the PR interval can vary with the heart rate (HR). In slow HR, the PR interval becomes longer. This is why, for example, in athletes, who may have a very slow resting HR (30-40 bpm), it’s normal to see a PR interval greater than 200 msec (1st-degree AV block). In the same vein, when the HR increases, the PR interval becomes shorter and can sometimes go down to 100 msec without indicating pre-excitation.
3. "A short PR interval indicates pre-excitation."
This statement is true.
Pre-excitation means that the ventricles are depolarised earlier than they should be. A typical cause of pre-excitation is Wolff-Parkinson-White (WPW) syndrome, which is beyond the scope of this post.
Why is this important? Because pre-excitation (like in WPW) can cause significant arrhythmias.
On the other hand, a prolonged PR interval indicates Atrio-Ventricular conduction delay. This means that there is an abnormal delay of conduction between the atria and ventricles.
Why is this important? Because abnormal AV conduction delay (known as AV block) can cause syncope, severe bradycardia, cardiac arrest, or it might be an indication of significant cardiac disease (depending on the severity of the AV block).
Click here to read more about AV conduction delay.
Summary
The PR interval is the period from the beginning of the P wave until the beginning of the QRS complex (excluding the QRS complex).
The physiological representation of the PR interval is the depolarisation of the atria (P wave) AND the depolarisation of the AV junction (AV node and His bundle).
The AV junction is the reason why there’s a delay between atrial and ventricular depolarisation and contraction. The delay is because of fewer gap junctions in the AV junction cells.
A prolonged PR interval indicates Atrio-Ventricular conduction delay.
A short PR interval indicates pre-excitation.
Further reading
Goldberger, A., Shvilkin, A. and Goldberger, Z. (no date) Goldberger’s Clinical Electrocardiography: A Simplified Approach. 9th ed. ELSEVIER.
Hall, J.E. and Hall, M.E. (2020) Guyton and Hall Textbook of Medical Physiology. 14th ed. Philadelphia, PA: Elsevier.
Drezner JA, Sharma S, Baggish A, Papadakis M, Wilson MG, Prutkin JM, Gerche A, Ackerman MJ, Borjesson M, Salerno JC, Asif IM, Owens DS, Chung EH, Emery MS, Froelicher VF, Heidbuchel H, Adamuz C, Asplund CA, Cohen G, Harmon KG, Marek JC, Molossi S, Niebauer J, Pelto HF, Perez MV, Riding NR, Saarel T, Schmied CM, Shipon DM, Stein R, Vetter VL, Pelliccia A, Corrado D. International criteria for electrocardiographic interpretation in athletes: Consensus statement. Br J Sports Med. 2017 May;51(9):704-731. doi: 10.1136/bjsports-2016-097331. Epub 2017 Mar 3. PMID: 28258178.